Acute HEV Infection Is a Relevant Cause of Decompensation and ACLF in Patients With Liver Cirrhosis.
Background and aims Hepatitis E virus (HEV) infection is very frequent in Europe with more than 2 million annual infections. Patients with liver cirrhosis may face an increased risk of suffering from acute-on-chronic liver failure (ACLF) due to HEV infection. We explored the consequences and prevalence of HEV infection in individuals with liver cirrhosis. Methods We retrospectively analysed the clinical outcome of all consecutive patients who were hospitalized at our center due to acute HEV infection and analysed their outcome between 2014 and 2024. Next, we tested 249 sera from 184 cirrhotic patients during individual episodes of acute hepatic decompensation for anti-HEV IgM and HEV-RNA to analyse the relevance of acute HEV infection as a triggering event. Finally, we established a single center cohort of patients with advanced liver cirrhosis, and assessed the anti-HEV IgG seroprevalence (n = 332). Results Over the past decade, 32 patients with liver cirrhosis who were hospitalized due to acute HEV infection were identified. Among these patients, 16 (50%) developed ACLF, resulting in five fatalities (31.3%) and three individuals (18.8%) requiring liver transplantation for survival. Of 249 sera obtained during acute hepatic decompensation, 11 (4.4%) were either HEV-RNA positive (n = 2) and/or anti-HEV IgM positive (n = 10), linking HEV infection to these acute decompensations. Screening of patients with liver cirrhosis for anti-HEV IgG showed that 67.2% of patients (223/332) were anti-HEV negative and thus at potential risk for future HEV infection. Conclusions Patients with advanced liver cirrhosis are at risk of acute HEV infection, which is a relevant cause of hepatic decompensation and ACLF with high mortality in these patients. Trial registration DRKS00010664; NCT04801290.
Introduction
Hepatitis E virus (HEV) infections are widespread in Germany, with an estimated 400 000 cases occurring annually [1]. Worldwide, it is the most prevalent cause of acute viral hepatitis and is responsible for significant morbidity and mortality, especially in regions with poor sanitation and contaminated water sources [2,3,4]. Furthermore, the increase in zoonotic transmission, particularly in developed countries where HEV genotypes (gt) 3 and 4 are associated with the consumption of undercooked meat, has gained relevance in recent years [3,5].
Four main genotypes of HEV have been identified as pathogenic to humans: Gt1‐4 [6]. In Germany, where this study was conducted, gt3 is the most prevalent genotype [7]. Infection with gt3 is typically asymptomatic and self‐limiting in healthy individuals. However, it can cause more severe disease, in particular in patients with underlying liver disease and chronic infection in immunosuppressed individuals, such as organ transplant recipients [2,8].
In contrast to the often self‐limiting nature of HEV in immunocompetent individuals, in whom the occurrence of acute liver failure is very rare, cirrhotic patients are at risk of developing ACLF, conditions associated with a mortality rate of over 30% [2,9,10,11,12,13]. Given the increasing number of deaths from cirrhosis in general, the burden of HEV in this population is a growing concern [14]. Patients with liver cirrhosis are more susceptible to infections, including HEV. This is believed to be due to their impaired liver function on the one hand, and the so‐called cirrhosis‐associated immune dysfunction (CAID) syndrome that involves systemic hyperinflammation and immune dysregulation on the other hand [15,16]. HEV superinfection in these patients often leads to rapid clinical deterioration characterized by worsening jaundice, ascites, encephalopathy, and coagulopathy [9,11,13].
Current clinical management of HEV infection in cirrhosis remains largely supportive, focusing on the treatment of complications associated with liver failure, such as ascites, acute kidney injury and hepatic encephalopathy [2,17,18]. Despite these interventions, outcomes in these patients are often poor, highlighting the need for novel therapeutic approaches to improve prognosis [11,19,20]. At present, there is no established antiviral treatment for acute HEV infection, and therapeutic options are limited, particularly for patients with advanced liver disease [2]. The antiviral drug ribavirin has demonstrated efficacy in the treatment of chronic HEV infection in immunocompromised patients, such as solid organ transplant recipients [2,21,22]. However, its role in acute HEV infection in cirrhotic patients remains unclear and has only been studied in a limited number of cases [23]. In addition, the potential for drug‐related toxicity such as anaemia and drug accumulation due to impaired kidney function in patients with liver cirrhosis further complicates its use in this population [24]. Consequently, there is a critical unmet need for more targeted and effective therapies to combat HEV infection in patients with cirrhosis, and subsequently prevent the onset of ACLF [13,19,25].
In this study, we aimed to assess the impact of HEV infection in patients with advanced liver cirrhosis at a large university hospital in northern Germany and to evaluate the clinical progression of the underlying condition in these individuals.
Patients and Methods
RNAExtraction andqPCR
Serum samples were mixed 1:2 with PBS and total nucleic acids were extracted from 500 μL using the AltoStar Purification Kit 1.5 (#PK15‐46) and the AltoStar Automation System AM16 from Altona diagnostics as instructed by the respected manufacturers' manuals. HEV‐RNA was then quantified with the AltoStar HEV‐RT‐PCR Kit 1.5 (#AS0271543) according to the manufacturer's instructions using the CFX96 Touch Real‐Time PCR Detection System (Bio‐Rad Laboratories, Hercules, CA).
Anti‐HEV IgM ELISA
WANTAI HEV IgM ELISA kits (#WANWE‐7196) were used for the detection of anti‐HEV IgM according to the manufacturer's protocol. Briefly, 10 μL of serum sample was added to 100 μL of diluent and incubated for 30 min at 37°C. The wells were washed 5 times with washing buffer and 100 μL of HRP‐conjugate was added and incubated for 30 min at 37°C following another 5 washes. 50 μL of colouring A and B were added for 15 min and stopped with the stop solution. Optical density was measured using the BioTek Synergy H1 Multimode Reader by Agilent at 450 nm and 630 nm as background. The cut off values were calculated using the average value of three negative controls or at least 0.03 plus 0.16. Samples were declared positive when the signal to cut‐off value was above 1.1 and negative when it was below 0.9.
Immunohistochemistry of Transjugular Liver Biopsies
Liver tissue from five out of the eight patients with HEV‐associated ACLF was available for immunohistochemistry analysis. As positive control we used a liver biopsy of a patient presenting with severe hepatitis due to acute viremic HEV infection (2.9 × 106IU/mL). A biopsy from a patient presenting with alcoholic liver disease related acute on chronic liver failure served as negative control. HEV infection was excluded in this case by PCR. Liver biopsies were processed into 2 μm sections, which were deparaffinized and stained on a Ventana Benchmark Ultra using a mouse anti‐hepatitis E monoclonal antibody (clone 1E6, Millipore MAB8002) with the OptiView detection kit. Stained sections were imaged using an Olympus BX43 microscope equipped with an Olympus DP23 camera.
Patients Included in This Study
All patients were seen at the Department of Gastroenterology, Hepatology, Infectious Diseases and Endocrinology at Hannover Medical School (MHH). The diagnosis of cirrhosis was based on clinical, radiological, or histological findings. ACLF was diagnosed according to the European Association for the Study of the Liver–Chronic Liver Failure (EASL‐CLIF) Consortium criteria [12,26]. Samples were obtained between August 2019 and April 2024 during routine blood draws and patients underwent no additional procedures for this study. Written informed consent was obtained from all participants before inclusion. The study was conducted in accordance with the ethical guidelines outlined in the Declaration of Helsinki. Sample collection and analysis of clinical data were approved by the Ethical Board of Hannover Medical School (12032‐Bo‐K‐2025, DRKS00010664, 3188‐2016;NCT04801290, 8498_BO_S_2019).
Statistical Analysis
Statistical analyses were performed using GraphPad Prism software 9.0 (GraphPad Software, San Diego, CA, USA) and SPSS (IBM Corp. Released 2023. IBM SPSS Statistics for Windows, Version 29.0.2.0 Armonk, NY, USA). For categorical variables, Fisher's exact test and for nominal variables Mann–WhitneyUtest were used to calculatepvalues. Details regarding statistical tests are displayed in the figure legends, and for all graphs, significances are indicated as *p< 0.05, **p< 0.01, ***p< 0.001, and ****p< 0.0001.
Results
Patient Cohort and Study Overview
To initially gain insight into the overall prevalence of HEV infection in patients with liver cirrhosis and assess its impact on the progression of the disease, we retrospectively analysed all patients hospitalized at the Hannover Medical School, Germany, between January 1, 2014 and August 31, 2024 that were tested positive for HEV‐RNA (n= 214, Figure1A). From these patients we specifically identified patients with liver cirrhosis and ACLF, and their outcomes were thoroughly examined.
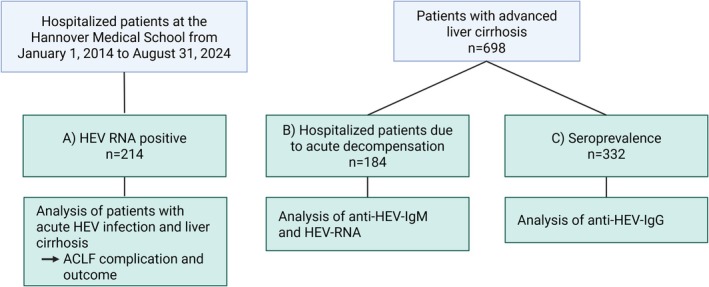
Study outline and overview of the cohorts analysed. The schematic summarizes the different patient cohorts (A–C) and analyses performed in this study.
Moreover, to investigate the role of acute HEV infection in the occurrence of acute decompensation, we analysed a bigger cohort of patients with advanced liver cirrhosis. To this end, we performed testing of both HEV‐RNA and anti‐HEV IgM in 184 patients of the prospective INFEKTA registry, including patients with ascites decompensated liver cirrhosis, at the time of hospitalization due to acute HEV infection (Figure1B).
Finally, to assess how many patients are at risk of HEV infection in an even bigger cohort of patients with advanced liver cirrhosis, we analysed the anti‐HEV IgG seroprevalence in 332 patients either enrolled in the INFEKTA registry or the Hannover TIPS cohort (Figure1C).
AcuteHEVInfection Leads to Severe Outcomes in Patients With Liver Cirrhosis
To better understand the course and complications of HEV infection in patients with liver cirrhosis, we retrospectively analysed all consecutive patients who were hospitalized at the Hannover Medical School from January 1, 2014 to August 31, 2024, with a positive HEV‐RNA test. Overall, 214 patients were identified, of whom 158 patients were diagnosed with acute HEV infection. Of the aforementioned cohort, 32 patients (20.3%) had a diagnosis of liver cirrhosis (Table2). Of these, 50% (n= 16) developed ACLF. During the course of their hospitalization, five patients (31.25%) died, and three patients (18.75%) underwent a rescue liver transplantation. Eight patients (50%) survived the ACLF and were discharged from the hospital after recovery (Figure2A, Table1). Moreover, the incidence of acute HEV infections has increased over time, with a marked surge in 2018 and 2019, followed by a plateau in the number of diagnosed cases thereafter (FigureS1).
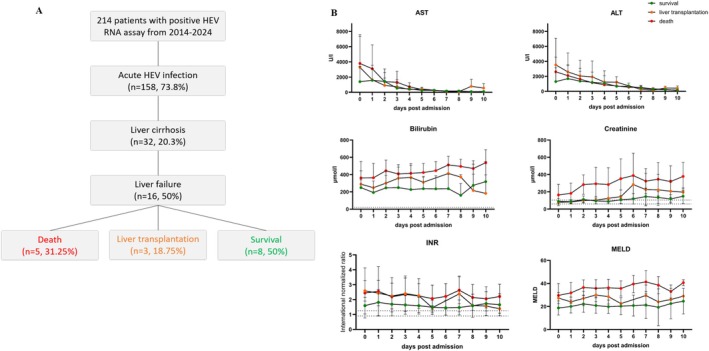
HEV infection in patients with liver cirrhosis leads to high morbidity and mortality. (A) Schematic of number of patients with HEV‐RNA positivity at MHH between 2014 and 2024. (B) Laboratory parameters of those patients during the first 10 days of admission to MHH. Dotted lines indicate norms.
Table: Baseline characteristics of patients with ACLF due to HEV infection between 2014 and 2024 at MHH.
Patients developing ACLF had significantly higher baseline values of bilirubin, international normalized ratio (INR), and the model of end‐stage liver disease (MELD) score as compared to those not developing ACLF (Table1). Additionally, hepatic encephalopathy and ascites decompensation were significantly increased in patients developing ACLF (Table1). Although not statistically significant, patients developing ACLF were about 3 years older, the percentage of male patients was higher, and more patients had diabetes mellitus II (Table1). Interestingly, a comparison of the underlying etiologies of liver cirrhosis revealed that patients who developed ACLF were more likely to have a steatotic liver disease compared to those who did not develop ACLF (Table1).
As anticipated, a comparison of HEV‐induced ACLF patients according to their outcome revealed that liver function was markedly compromised in patients who died or required a rescue liver transplantation, in comparison to those who survived ACLF (Table1, Figure2B). In more detail, on the day of admission the MELD score was significantly elevated in patients who died or needed rescue liver transplantation in comparison to patients that survived without the need for transplantation (Table1). Noteworthy, during the first 10 days upon admission to hospital, there were only minor differences in the kinetics of laboratory parameters between patients who survived ACLF and those who died or underwent liver transplantation (Figure2B). While the liver enzymes alanine transaminase (ALT) and aspartate aminotransferase (AST) exhibited a rapid decline across all groups, INR, bilirubin, and creatinine levels remained elevated (Figure2B). This aligns with the MELD score, which was highest among the ACLF‐related fatalities and did not change over time (Table1, Figure2B). HEV‐related mortality cases are characterized in TableS1. In more detail, aetiology of cirrhosis was predominantly steatotic liver disease. Two out of eight patients received ribavirin treatment and transjugular liver biopsy was performed in five patients (TableS1). Noticeably, in all of the available biopsies, the capsid protein of HEV, ORF2 was detectable upon immunohistochemical staining, confirming the infection of HEV in the liver of these patients (FigureS3).
In summary, a total of 16 cases of ACLF due to acute HEV infection were identified over the past decade at a university hospital in Germany, which is half of the cirrhotic patients hospitalized with HEV infection. Of these patients, 50% died or needed a life‐saving liver transplantation.
HEVInfection Is a Relevant Cause of Acute Decompensation in Patients With Liver Cirrhosis
After having established that HEV infection leads to the development of ACLF with high case‐fatality rates in patients with liver cirrhosis, we wanted to investigate whether acute HEV infection is a relevant cause of hospitalization due to acute decompensation in patients with liver cirrhosis and explore how often it might be overlooked as an underlying cause of acute decompensation.
Therefore, we tested 249 serum samples of 184 patients that suffered from acute hepatic decompensation for HEV‐RNA (FigureS2, TablesS2andS3). The earliest available sample from each hospitalization due to acute decompensation, as defined by the manifestation of ascites, hepatic encephalopathy, oesophageal varices bleeding, and/or occurrence of icterus [27,28] was obtained. 62 patients exhibited multiple events and multiple samples were tested. Of the 249 samples from 184 patients tested, two were found to contain HEV‐RNA, representing a prevalence of 1.1% (TableS2). Interestingly, in one of those two patients, HEV infection was not diagnosed during the course of hospitalization.
To further exclude the possibility of missed cases due to HEV‐RNA being already cleared from the serum, an additional test for anti‐HEV IgM, indicative of recent HEV infection, was conducted on these sera. Of the 249 samples tested, 13 samples (5.22%) from 10 patients were identified as positive for anti‐HEV IgM. In three patients, the samples from two subsequent events with a time of 1–3 months in between presented as anti‐HEV IgM positive (TableS3, patient ID 107, 137, 177). When only considering the first anti‐HEV IgM positive sample per patient, this results in an anti‐HEV IgM prevalence of 5.4% (10/184; TablesS2andS3). While in two patients, the anti‐HEV IgM ELISA signal to cut‐off (S/CO) values were low and rather stable over time (ID 137, 177), the third patient (ID 107) had a notable increase in S/CO values, highly indicative of a recent infection with HEV (TableS3). One of two HEV‐RNA positive samples was also anti‐HEV IgM positive (TableS3). Taken together, 11 of 249 (4.4%) hospitalizations due to acute decompensation in patients with liver cirrhosis could be linked to HEV infection.
When comparing the laboratory parameters of the full cohort of patients with hepatic decompensation (n= 698) to those whose decompensation was associated with recent HEV infection (n= 11), there were no significant differences between the two groups. The only noticeable difference was a slight elevation in bilirubin concentrations in the HEV‐related cases relative to the overall cohort (Figure3). Overall, the small number of HEV‐associated decompensations limits the robustness of these observations.
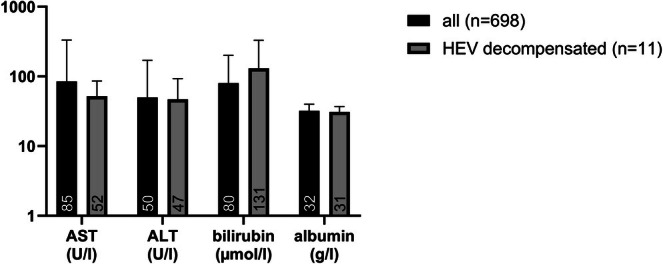
Laboratory parameters in hospitalizations in cirrhosis patients due to acute decompensation linked to acute HEV infection. The graph depicts the laboratory parameters of the 11 decompensations that were either HEV‐RNA or anti‐HEV IgM positive and those of the overall cohort. ALT, alanine transaminase; AST, aspartate aminotransferase.
Seroprevalence of Anti‐HEV IgGAntibodies in Patients With Advanced Liver Cirrhosis
Results of anti‐HEV IgG testing using the Wantai anti‐HEV IgG assay were available in 332 patients (Table2) of the whole study cohort. Interestingly, of the 332 patients, 109 (32.8%) were positive for anti‐HEV IgG (Table2). This indicates that in our cohort of patients with advanced liver cirrhosis, one third had a previous or possibly ongoing HEV infection.
Table: Patient characteristics and HEV seroprevalence.
With the results of this large cohort, we sought to determine if there were any risk factors associated with anti‐HEV IgG positivity. Notably, we observed that anti‐HEV IgG positive patients were significantly older compared to patients who were negative for anti‐HEV IgG (Table2). As expected, patients with cirrhosis were more likely to be male than female in both groups, whereas there were no significant gender differences between anti‐HEV IgG positive and anti‐HEV IgG negative patients (Table2). Moreover, severity of liver cirrhosis, as assessed by laboratory values, onset of hepatic encephalopathy, ascites decompensation, and the MELD score, was comparable between anti‐HEV IgG positive and anti‐HEV IgG negative patients (Table2).
Comparing the different etiologies of liver cirrhosis in the two groups, we observed that cirrhosis was more often related to steatotic liver disease, and the percentages were even significantly higher in the anti‐HEV IgG positive group, whereas chronic hepatitis virus infections, such as hepatitis B, C, and D, were significantly more common in anti‐HEV IgG negative patients (Table2). Of note, autoimmune hepatitis was more common as the underlying cause of cirrhosis in anti‐HEV IgG negative patients; however, it failed to reach statistical significance (Table2).
Taken together, the seroprevalence of anti‐HEV IgG antibodies in patients with advanced liver cirrhosis is substantial, emphasizing the relevance of acute HEV infection in these patients. Importantly, 223 (67.2%) of the patients were anti‐HEV IgG negative and thus at potential risk of infection and subsequent development of acute decompensation or ACLF, ultimately leading to high mortality.
Discussion
In this study, we analysed the risk and implications of HEV infection in patients with advanced liver cirrhosis, using different patient cohorts and combining both clinical data as well as further testing of patient samples for HEV‐RNA and anti‐HEV IgM.
Overall, we identified 32 patients with acute HEV infection and underlying liver disease treated in the past decade at Hannover Medical School, half of which developed ACLF. Patients with liver cirrhosis are susceptible to bacterial, fungal, and viral superinfections due to an immune dysfunctional state [29]. Having observed that patients with liver cirrhosis are at risk of acute HEV infection and are subsequently susceptible to develop ACLF, one may speculate that CAID in cirrhosis patients may contribute to disease severity in these patients due to dysregulated immune responses [4,30].
Based on the prevalence of different HEV gt, most likely all patients included in this study were infected with gt3 HEV. Gt1 and gt2 are more prevalent in Asia and developing countries and can cause outbreaks due to human‐to‐human transmission via contaminated water supplies (recent outbreak in South Sudan) [31]. Overall, the disease burden including the occurrence of acute liver failure (ALF) is higher in gt1 and gt2 infections, resulting in elevated case fatality rates [18,32,33].
Of these 16 observed cases of ACLF, half (50%) did not survive or survived only because of liver transplantation. This is in line with a previously published study showing short‐term mortality rates of HEV‐related ACLF ranging from 0% to 67% with a median of 34% [10]. These high mortality rates indicate an urgent need for new therapeutic options to prevent acute HEV infection in patients with liver cirrhosis and subsequently avoid the onset of ACLF and death [4,19].
Interestingly, we were able to find a link to recent HEV infection in 4% (10/249) of hospitalisations due to acute hepatic decompensations. These findings emphasise the substantial underestimation of HEV infection within this patient cohort. Despite the fact that all patients received treatment at a tertiary care facility and university hospital, our testing of 249 serum samples for HEV‐RNA positivity revealed two HEV‐RNA positive samples, of which one was overlooked during hospitalisation. Notably, this case occurred in 2020, a period when HEV infection was recognised as a potential cause of acute decompensation that warranted testing. For example, the European association for the study of the liver (EASL) recommended to test blood products for HEV‐RNA positivity already in 2018 [2,34]. This increased awareness might also be causal of the increased cases of acute HEV infection over the course of the years between 2014 and 2024 that peaked in 2019 (FigureS2). Testing the same cohort for anti‐HEV IgM positivity hinted to a relevant number of additional cases of acute decompensations due to HEV infection. While studies have shown the persistence of anti‐HEV IgM positivity for a longer period of time after spontaneous viral clearance [35], a possible recently cleared HEV infection as cause for the acute decompensation in these patients cannot be ruled out. Therefore, a significant number of undetected cases should be taken into account when considering the total number of acute decompensation and ACLF cases attributed to HEV infection, as highlighted in our study and other previously published research [36].
The anti‐HEV IgG seroprevalence in our cohort was 32.8%, markedly higher than that observed in the general population [1]. Although variations in the serological assays used should be taken into account, these differences remain relevant when assessing both the prevalence and clinical impact of HEV infection in this specific cohort of patients with decompensated liver cirrhosis, who are vulnerable to infections. Additionally, it is important to note that over 60% of cirrhotic patients in our cohort were anti‐HEV IgG negative, putting them at risk of future HEV infection. While the extent and duration of protection conferred by anti‐HEV IgG positivity against HEV infection remains unclear, it is noteworthy that all identified HEV infections occurred in patients who were previously negative for anti‐HEV IgG.
In conclusion, this study demonstrates that patients with liver cirrhosis are at high risk of acute HEV infection. Indeed, we were able to link 4% of hospitalizations due to acute decompensation to a recent HEV infection. Moreover, these patients are particularly vulnerable to developing subsequent complications such as acute decompensation and/or ACLF, which ultimately lead to high mortality rates. Further studies are urgently needed to investigate new preventive and therapeutic options to target acute HEV infection in patients with liver cirrhosis and subsequently prevent the onset of ACLF.
Author Contributions
The study was designed by B.M., P.B., K.D., and C.N. Patients were recruited by B.M., M.C., A.R.M.K., H.W., and K.D. Experiments were performed by K.D., B.B., C.W., and N.P. Data analysis and statistics were performed by K.D., C.N., and A.T. Drafting of the manuscript was done by B.M., P.B., K.D., and C.N. All authors had access to the study data and reviewed and approved the final manuscript.
Funding
K.D. was supported by a Clinical Leave stipend of the German Centre for Infection Research (DZIF, TI 07.001_005). H.W., M.C., P.B. and B.M. were funded by a grant from the German Centre for Infection Research (DZIF). A.D. was supported by the KlinStrucMed Programme of Hannover Medical School. A.D. and B.M. were supported by the MHH plus foundation of Hannover Medical School. H.W. was funded by the German Ministry of Education and Research (HepEDiaSeq 01EK2106A/B).
Ethics Statement
Sample collection and analysis of clinical data was approved by the Ethical Board of Hannover Medical School (12032‐Bo‐K‐2025, DRKS00010664, 3188‐2016;NCT04801290, 8498_BO_S_2019).
Consent
Written informed consent was obtained from all participants before inclusion.
Conflicts of Interest
Katja Dinkelborg: nothing to disclose; Christian Niehaus: nothing to disclose; Birgit Bremer: nothing to disclose; Christine Wundes: nothing to disclose; Anja Tiede: nothing to disclose; Natalie Petruch: nothing to disclose; Katja Deterding: travel support and research grant from Gilead. Speaker fees from Gilead and Alnylam. Advisory board member: Gilead. Anke R.M. Kraft: nothing to disclose; Björn Hartleben: nothing to disclose; Markus Cornberg: advises and is on the speakers' bureau for AbbVie and Gilead, advises AiCuris, GSK and Roche. He is on the speakers' bureau for Falk. Heiner Wedemeyer: served as a speaker/advisory board member for Abbott Laboratories and Abbott Molecular Inc., Bristol‐Myers‐Squibb, Gilead Sciences GmbH and Gilead Sciences Ltd., GlaxoSmithKline Services Unlimited, Janssen, Roche Diagnostics International Ltd., Vir Biotechnology Inc., received research support from Abbott Laboratories and Abbott Molecular Inc., Biotest AG and received lecture fees from Biotest AG and Gilead Sciences GmbH and Gilead Sciences Ltd. Patrick Behrendt: nothing to disclose; Benjamin Maasoumy: served as a speaker and/or advisory board member for AbbVie, AstraZeneca, EWIMED, Fujirebio, Gilead, Luvos, MSD, Norgine, Roche and W.L. Gore and Associates and received research support from Altona, EWIMED, Fujirebio and Roche.
References
- M. Faber, N. Willrich, M. Schemmerer, et al. , “Hepatitis E Virus Seroprevalence, Seroincidence and Seroreversion in the German Adult Population, ”Journal of Viral Hepatitis25(2018): 752–758. doi.org/10.1111/jvh.12868
- European Association for the Study of the Liver, “EASL Clinical Practice Guidelines on Hepatitis E Virus Infection, ”Journal of Hepatology68(2018): 1256–1271. doi.org/10.1016/j.jhep.2018.03.005
- S. Kumar, S. Subhadra, B. Singh, andB. K. Panda, “Hepatitis E Virus: The Current Scenario, ”International Journal of Infectious Diseases17(2013): e228–e233. doi.org/10.1016/j.ijid.2012.11.026
- Y. Brüggemann, M. Klöhn, H. Wedemeyer, andE. Steinmann, “Hepatitis E Virus: From Innate Sensing to Adaptive Immune Responses, ”Nature Reviews. Gastroenterology & Hepatology21(2024): 710–725. doi.org/10.1038/s41575-024-00950-z
- E. J. Aspinall, E. Couturier, M. Faber, et al. , “Hepatitis E Virus Infection in Europe: Surveillance and Descriptive Epidemiology of Confirmed Cases, 2005 to 2015, ”Euro Surveillance22(2017): 30561. doi.org/10.2807/1560-7917.ES.2017.22.26.30561
- L. Kamani, Z. A. Padhani, andJ. K. Das, “Hepatitis E: Genotypes, Strategies to Prevent and Manage, and the Existing Knowledge Gaps, ”JGH Open5(2021): 1127–1134. doi.org/10.1002/jgh3.12646
- M. Schemmerer, J. J. Wenzel, K. Stark, andM. Faber, “Molecular Epidemiology and Genotype‐Specific Disease Severity of Hepatitis E Virus Infections in Germany, 2010‐2019, ”Emerging Microbes & Infections11(2022): 1754–1763. doi.org/10.1080/22221751.2022.2091479
- N. Kamar, L. Rostaing, andJ. Izopet, “Hepatitis E Virus Infection in Immunosuppressed Patients: Natural History and Therapy, ”Seminars in Liver Disease33(2013): 62–70. doi.org/10.1055/s-0033-1338115
- T. ‐C. Tseng, C. ‐J. Liu, C. T. Chang, et al. , “HEV Superinfection Accelerates Disease Progression in Patients With Chronic HBV Infection and Increases Mortality in Those With Cirrhosis, ”Journal of Hepatology72(2020): 1105–1111. doi.org/10.1016/j.jhep.2020.01.012
- A. KumarandV. A. Saraswat, “Hepatitis E and Acute‐On‐Chronic Liver Failure, ”Journal of Clinical and Experimental Hepatology3(2013): 225–230. doi.org/10.1016/j.jceh.2013.08.013
- J. W. Choi, H. J. Son, S. S. Lee, et al. , “Acute Hepatitis E Virus Superinfection Increases Mortality in Patients With Cirrhosis, ”BMC Infectious Diseases22(2022): 62. doi.org/10.1186/s12879-022-07050-w
- R. Hernaez, E. Solà, R. Moreau, andP. Ginès, “Acute‐On‐Chronic Liver Failure: An Update, ”Gut66(2017): 541–553. doi.org/10.1136/gutjnl-2016-312670
- M. Buti, J. C. Ruiz‐Cobo, R. Esteban, andM. Riveiro‐Barciela, “Hepatitis E as a Trigger for Acute‐On‐Chronic Liver Failure, ”Clinical and Molecular Hepatology31(2025): S196–S204. doi.org/10.3350/cmh.2024.0758
- D. Q. Huang, N. A. Terrault, F. Tacke, et al. , “Global Epidemiology of Cirrhosis — Aetiology, Trends and Predictions, ”Nature Reviews Gastroenterology & Hepatology20(2023): 388–398. doi.org/10.1038/s41575-023-00759-2
- A. Albillos, M. Lario, andM. Álvarez‐Mon, “Cirrhosis‐Associated Immune Dysfunction: Distinctive Features and Clinical Relevance, ”Journal of Hepatology61(2014): 1385–1396. doi.org/10.1016/j.jhep.2014.08.010
- A. Albillos, R. Martin‐Mateos, S. Van der Merwe, et al. , “Cirrhosis‐Associated Immune Dysfunction, ”Nature Reviews Gastroenterology & Hepatology19(2022): 112–134. doi.org/10.1038/s41575-021-00520-7
- H. Wedemeyer, S. Pischke, andM. P. Manns, “Pathogenesis and Treatment of Hepatitis e Virus Infection, ”Gastroenterology142(2012): 1388–13970. doi.org/10.1053/j.gastro.2012.02.014
- T. Horvatits, J. Schulze zur Wiesch, M. Lütgehetmann, A. W. Lohse, andS. Pischke, “The Clinical Perspective on Hepatitis E, ”Viruses11(2019): 617. doi.org/10.3390/v11070617
- K. Ullah, A. W. Dogar, S. Ochani, andH. B. Ahmad, “Hepatitis E Infection in Chronic Liver Disease Patients Causing Acute on Chronic Liver Failure: Vaccination Is Need of the Hour, ”BMJ Open Gastroenterology9(2022): e001051. doi.org/10.1136/bmjgast-2022-001051
- P. BehrendtandH. Wedemeyer, “Impfstoffe gegen Hepatitis E: Wo stehen wir?, ”Bundesgesundheitsblatt, Gesundheitsforschung, Gesundheitsschutz65(2022): 192–201. doi.org/10.1007/s00103-022-03487-1
- N. Kamar, J. Izopet, S. Tripon, et al. , “Ribavirin for Chronic Hepatitis E Virus Infection in Transplant Recipients, ”New England Journal of Medicine370(2014): 1111–1120. doi.org/10.1056/NEJMoa1215246
- N. Kamar, F. Abravanel, P. Behrendt, et al. , “Ribavirin for Hepatitis E Virus Infection After Organ Transplantation: A Large European Retrospective Multicenter Study, ”Clinical Infectious Diseases71(2019): 1204–1211. doi.org/10.1093/cid/ciz953
- J. M. Péron, H. Dalton, J. Izopet, et al. , “Acute Autochthonous Hepatitis E in Western Patients With Underlying Chronic Liver Disease: A Role for Ribavirin?, ”Journal of Hepatology54(2011): 1323–1324. doi.org/10.1016/j.jhep.2011.01.009
- A. GoelandR. Aggarwal, “Advances in Hepatitis E – II: Epidemiology, Clinical Manifestations, Treatment and Prevention, ”Expert Review of Gastroenterology & Hepatology10(2016): 1065–1074. doi.org/10.1080/17474124.2016.1185365
- M. Frias, P. López‐López, A. Rivero, andA. Rivero‐Juarez, “Role of Hepatitis E Virus Infection in Acute‐On‐Chronic Liver Failure, ”BioMed Research International2018(2018): 9098535. doi.org/10.1155/2018/9098535
- R. Moreau, R. Jalan, P. Gines, et al. , “Acute‐On‐Chronic Liver Failure Is a Distinct Syndrome That Develops in Patients With Acute Decompensation of Cirrhosis, ”Gastroenterology144(2013): 1426–1437. doi.org/10.1053/j.gastro.2013.02.042
- E. A. Tsochatzis, J. Bosch, andA. K. Burroughs, “Liver Cirrhosis, ”Lancet383(2014): 1749–1761. doi.org/10.1016/S0140-6736(14)60121-5
- G. D'Amico, M. Bernardi, andP. Angeli, “Towards a New Definition of Decompensated Cirrhosis, ”Journal of Hepatology76(2022): 202–207. doi.org/10.1016/j.jhep.2021.06.018
- S. Piano, C. Bunchorntavakul, S. Marciano, andK. Rajender Reddy, “Infections in Cirrhosis, ”Lancet Gastroenterology & Hepatology9(2024): 745–757. doi.org/10.1016/S2468-1253(24)00078-5
- J. Wu, B. Ling, N. Guo, G. Zhai, M. Li, andY. Guo, “Immunological Manifestations of Hepatitis E‐Associated Acute and Chronic Liver Failure and Its Regulatory Mechanisms, ”Front Med (Lausanne)8(2021): 725993. doi.org/10.3389/fmed.2021.725993
- G. S. Orf, N. Bbosa, M. G. Berg, et al. , “The 2023 South Sudanese Outbreak of Hepatitis E Emphasizes Ongoing Circulation of Genotype 1 in North, Central, and East Africa, ”Infection, Genetics and Evolution124(2024): 105667. doi.org/10.1016/j.meegid.2024.105667
- D. B. Rein, G. A. Stevens, J. Theaker, J. S. Wittenborn, andS. T. Wiersma, “The Global Burden of Hepatitis E Virus Genotypes 1 and 2 in 2005, ”Hepatology55(2012): 988–997. doi.org/10.1002/hep.25505
- M. S. Hakim, W. Wang, W. M. Bramer, et al. , “The Global Burden of Hepatitis E Outbreaks: A Systematic Review, ”Liver International37(2017): 19–31. doi.org/10.1111/liv.13237
- F. Boland, A. Martinez, L. Pomeroy, andN. OFlaherty, “Blood Donor Screening for Hepatitis E Virus in the European Union, ”Transfusion Medicine and Hemotherapy46(2019): 95–103. doi.org/10.1159/000499121
- M. Riveiro‐Barciela, A. Rando‐Segura, A. Barreira‐Díaz, et al. , “Unexpected Long‐Lasting Anti‐HEV IgM Positivity: Is HEV Antigen a Better Serological Marker for Hepatitis E Infection Diagnosis?, ”Journal of Viral Hepatitis27(2020): 747–753. doi.org/10.1111/jvh.13285
- G. Buescher, A. ‐K. Ozga, E. Lorenz, et al. , “Hepatitis E Seroprevalence and Viremia Rate in Immunocompromised Patients: A Systematic Review and Meta‐Analysis, ”Liver International41(2021): 449–455. doi.org/10.1111/liv.14695
Republished from the open web under CC-BY. Authors: Dinkelborg K, Niehaus C, Bremer B, Wundes C, Tiede A, Petruch N, Deterding K, Kraft ARM, Hartleben B, Cornberg M, Wedemeyer H, Behrendt P, Maasoumy B. Read the original.