Dietary Phytochemical Index and Its Relationship With Diminished Ovarian Reserve: Evidence From a Case-Control Study.
Introduction Diminished ovarian reserve (DOR) represents a significant contributor to female infertility and adverse reproductive outcomes. Although diet may play a role, the specific impact of phytochemical-rich dietary patterns remains underexplored. So, we aimed to investigate the association between adherence to a dietary phytochemical index (DPI) and the likelihood of DOR among women attending fertility clinics. Methods This case-control study enrolled 370 women, comprising 120 individuals diagnosed with DOR and 250 age- and body mass index (BMI)-matched controls with normal ovarian reserve. A validated semi-quantitative food frequency questionnaire (FFQ) was applied to assess dietary intakes and, accordingly, DPI was calculated as the proportion of total energy intake obtained from phytochemical-abundant foods. Antral follicle count (AFC) and serum anti-Müllerian hormone (AMH) measurements were utilized as indicators of ovarian reserve. The association between DPI and the odds of DOR was investigated using multivariable logistic regression models. Results Our findings showed that higher DPI was associated with a reduced odds of DOR (Q4 vs. Q1 OR: 0.79; 95% CI: 0.55-0.93; p-trend = 0.010). After adjustment for physical activity and energy intake, the association remained significant (OR: 0.80; 95% CI: 0.54-0.95; p-trend = 0.033). In the fully adjusted model, which included additional adjustments for fat mass and body mass index, women in the highest DPI quartile had 27% lower odds of DOR compared to those in the lowest quartile (OR: 0.73; 95% CI: 0.42-0.97; p-trend = 0.02). Besides, in the control group, AFC differed significantly across DPI quartiles (p Conclusion Our findings suggest that a phytochemical-rich diet may help reduce the odds of DOR, highlighting the role of diet in reproductive health. However, further prospective studies and mechanistic research are warranted to confirm these results and clarify underlying pathways.
Introduction
Ovarian reserve, which reflects the number and quality of the remaining ovarian follicles in a woman's ovaries, is a critical contributor to ovarian function [1]. Diminished ovarian reserve (DOR), which happens when this reserve declines to lower than expected for a woman's age, serves as a crucial predictor of fertility capacity, the ovarian response to assisted reproductive treatments, reproductive years, and the possible age at menopause [2]. Anti‐Müllerian hormone (AMH), secreted by granulosa cells of early antral follicles, and antral follicle count (AFC), assessed via transvaginal ultrasound, are currently recognised as the most promising quantitative markers of ovarian reserve [3]. Although ovarian reserve decreases with advancing age, considerable variations are observed among women of the same age group, which highlight significant interindividual differences [4]. These variabilities propose that beyond chronological age, additional determinants may influence the rate and degree of ovarian reserve decline [2].
Despite the well‐established role of advancing age in the determination of depletion of the ovarian oocyte pool, this process is also influenced by a complex interaction of factors including genetic predisposition, gynaecological conditions (e.g., endometriosis, tumours, infections, and prior ovarian surgery), environmental exposures (such as endocrine‐disrupting substances), and lifestyle‐related factors like psychological stress and, in particular, diet [4,5]. Among these, diet has gained considerable attention due to its modulatory effects on oxidative stress, inflammation, and endocrine function, all of which play crucial roles in female reproductive health [6].
Considering nutritional factors, emerging evidence highlights the favourable effects of healthy dietary patterns such as the Mediterranean diet, characterised by high intake of vegetables and fruit, nuts, legumes, olive oil, fish, and whole grains, and low consumption of red and processed meats, sweets, and saturated fats, on fertility outcomes [7,8]. The positive impact of these plant‐based diets may be attributed to their abundant content of essential nutrients and bioactive compounds such as vitamins, minerals, dietary fibre, and phytochemicals [9]. Phytochemicals are non‐nutritive bioactive substances, including polyphenols, carotenoids, phytosterols, and organosulfur compounds that are widely found in fruits, vegetables, nuts, whole grains, herbs and beverages such as tea and wine [10]. The likely reproductive health‐promoting effects of phytochemicals have been shown in previous epidemiological investigations across various populations [11,12]. These natural compounds exert their benefits mainly by regulating oxidative stress, managing inflammation, and maintaining hormonal balance [13]. However, the majority of prior research on phytochemical intake has focused on individual nutrients, foods, or food groups [11,14], while by comparison less attention has been given to comprehensive frameworks that assess the broader impact of phytochemical‐rich food combinations in the context of reproductive health and productivity.
Dietary Phytochemical Index (DPI) calculation provides a simple, cost‐effective approach to assess phytochemical intake and overall dietary quality [15]. Despite certain limitations, it could be applied in clinical practice [15]. DPI has attracted interest as a potentially modifiable factor in female reproductive health, supported by previous studies reporting inverse associations between DPI adherence and reproductive disorders such as polycystic ovary syndrome (PCOS) [16,17]. Nonetheless, a significant knowledge gap remains regarding the specific association between this index and ovarian reserve status. As such, to shed light on this significant but neglected area, we aimed to investigate the potential relationship between DPI and the odds of having DOR in women attending fertility clinics.
Methods
Study Design and Participants
This research was conducted as a case–control study involving a total of 370 Iranian women, comprising 120 individuals diagnosed with DOR and 250 women with normal ovarian function serving as controls. We adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines in reporting this observational study. Participants were selected from infertility clinics associated with Isfahan University of Medical Sciences. Eligible women were between 18 and 45 years of age, with a body mass index (BMI) ranging from 20 to 35 kg/m2. Diagnosis of DOR was confirmed by two gynaecologists using criteria based on serum AMH levels of ≤ 0.7 ng/mL and/or an AFC of ≤ 4 [18]. To minimise misclassification and distinguish DOR from perimenopause or premature ovarian insufficiency (POI), women with clinical indicators suggestive of early ovarian decline such as prolonged or persistent menstrual irregularity and characteristic vasomotor symptoms (e.g., hot flashes and night sweats) were excluded from the study [19]. Frequency matching was applied to ensure similar distributions of important confounders between cases and controls. Specifically, cases and controls were matched based on age and BMI categories to minimise potential confounding. The required sample size for this study was estimated using standard formulas for unmatched case–control designs. Although cases and controls were matched on key characteristics in the study design, using the unmatched formula provides a conservative estimate of the required sample size, as matched designs typically increase statistical efficiency. Calculations were based on a two‐sided test, a 95% confidence level (α = 0.05), and 80% statistical power (β = 0.20). An anticipated odds ratio (OR) of 0.50 was assumed, reflecting a hypothesized 50% lower odds of DOR among women in the highest quartile of the DPI, based on previous evidence suggesting protective effects of phytochemical‐rich diets on reproductive health [17,20]. The proportion of exposure (high DPI) among the control group was derived from our preliminary data, in which approximately 25% of control participants were categorised in the highest DPI quartile. The minimum required sample size was estimated at approximately 91 cases and 182 controls (273 participants in total). To account for an expected 10% non‐response or exclusion rate, the final target sample size was increased to 370 participants, including 120 women with DOR and 250 controls.
Individuals with a history of ovarian surgery, endometriosis, radiotherapy, chemotherapy, hormonal treatment, or special diets in the previous 3 months were excluded. Additionally, participants with endocrine or metabolic conditions were not eligible. Informed consent was obtained from all subjects, and the study protocol was approved by the Ethics Committee of Isfahan University of Medical Sciences (IR.ARI.MUI.REC.1401.297).
Dietary assessment and phytochemical index calculation
Dietary data were collected using a validated semi‐quantitative food frequency questionnaire (FFQ) containing 80 items [21]. Trained nutritionists conducted face‐to‐face interviews to complete the FFQs. Standard household measures were used to convert portion sizes into grams [22], and the Iranian‐adapted Nutritionist IV software was employed to analyse nutrient intake [23].
To better understand how phytochemical mixtures in the human diet contribute to health outcomes, researchers formulated the DPI, which represents the percentage of total daily calories consumed from foods rich in phytochemicals [24]. The DPI was calculated using the following formula [24]:
DPI = [daily energy obtained from foods rich in phytochemicals (kcal)/total daily energy intake (kcal) × 100].
Fruits, vegetables, legumes, whole grains, nuts, soy products, seeds, and olive oil were identified as primary sources of dietary phytochemicals and were therefore included in the DPI calculation. Foods such as potatoes, pickled vegetables, and vegetable powders were excluded due to their limited phytochemical content. Natural fruit juices were grouped with fruits, while vegetable juices and tomato‐based sauces were classified as vegetables, given their substantial phytochemical content, and all were incorporated into the DPI assessment. Following the calculation, DPI scores were divided into quartiles, with individuals in the highest quartile reflecting the greatest intake of phytochemical‐rich foods.
Anthropometric and Clinical Measures
Body weight and height were measured using calibrated instruments, and BMI was computed as weight in kilograms divided by height in meters squared. Waist circumference (WC) and hip circumference (HC) were measured to calculate the waist‐to‐hip ratio (WHR). Fat mass (FM) and fat‐free mass (FFM) were assessed using bioelectrical impedance analysis (InBody 770). Systolic and diastolic blood pressures were recorded using an automated digital monitor after participants rested for 15 min. Physical activity levels were assessed with the validated Iranian version of the International Physical Activity Questionnaire (IPAQ), reported in metabolic equivalent hours per day (MET‐h/day) [25]. Serum AMH levels were measured using ELISA kits (Monobind, California, USA), according to the manufacturer protocols, and AFC was evaluated using transvaginal ultrasonography on the third day of a spontaneous menstrual cycle.
Statistical Analysis
Continuous variables in this study were presented as means and standard deviations (SD), and differences between groups were analysed using the independent samplet‐test and one‐way ANOVA. Categorical data were summarised as frequencies (%), and the chi‐square test was used to assess differences between the case and control groups. Logistic regression analysis was conducted to estimate the ORs and 95% confidence intervals (CIs) for DOR across DPI quartiles. Model 1 was adjusted for physical activity and calorie intake; Model 2 additionally adjusted for BMI and fat mass. All analyses were conducted using SPSS version 22 (IBM Corp, Armonk, NY, USA). Statistical significance was determined forp‐values below 0.05.
Results
In this study, 120 women diagnosed with DOR were recruited as the case group, and 250 age‐ and BMI‐matched women with normal ovarian reserve were enrolled as the control group. A total of 382 women were initially recruited. Nonetheless, 12 participants were excluded from the study: 6 due to unwillingness to participate and 6 due to incomplete questionnaire responses (Figure1). The baseline characteristics of participants are presented in Table1. Women with DOR had significantly higher FM (38.47 vs. 36.47 kg,p= 0.020), WC (102.23 vs. 91.70 cm,p= 0.002), and WHR (0.90 vs. 0.86,p= 0.003), and significantly lower AFC (2.34 vs. 9.59,p< 0.001) and AMH levels (0.56 vs. 4.11 ng/mL, p < 0.001), compared to controls.
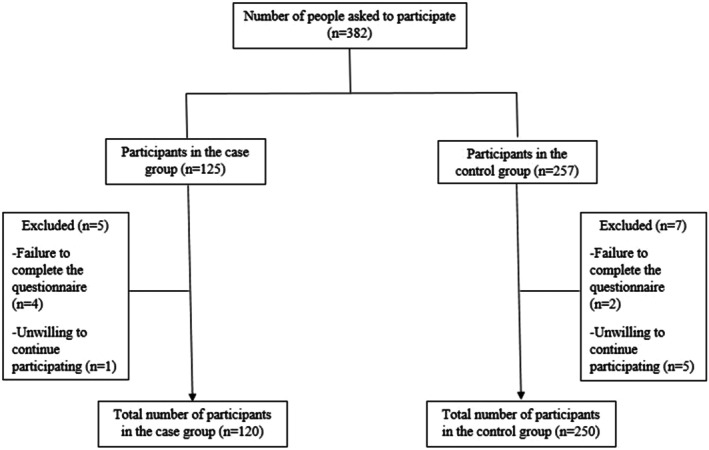
Flowchart of participant selection and study enrollment. Participants were 4 matched based on age and BMI at the time of recruitment to control for baseline confounders.
Table: Baseline characteristic of study participants.
Table2summarises the demographic, anthropometric, and clinical characteristics of participants across quartiles of the DPI, separately for case and control groups. No statistically significant differences were found across DPI quartiles with respect to age, BMI, WC, fat mass, or fat‐free mass (p> 0.05) in either the case or control group. However, among the control group, the AFC differed significantly across DPI quartiles (p< 0.001), with the highest mean count observed in the second quartile.
Table: Characteristic of study participants according to quartiles of DPI.
Table3presents dietary intake profiles across DPI quartiles. As expected, higher DPI scores were consistently associated with healthier dietary patterns in both groups. Among controls, total energy, protein, carbohydrate, and fat intakes increased significantly across DPI quartiles (p< 0.001). Intake of phytochemical‐rich foods such as fruits, vegetables, legumes, nuts, whole grains, olives, soy, tea, and spices showed a clear increasing trend with higher DPI scores (allp< 0.001). Participants in the highest DPI quartile consumed significantly more fruits (589 ± 425 g/day), vegetables (648 ± 402 g/day), legumes, whole grains, soy, and tea compared to those in the lowest quartile (allp< 0.001). Saturated fat intake remained relatively stable in controls. However, among patients with DOR, those assigned to the highest quartile had a higher consumption of SFA in comparison with the lowest category (p< 0.001).
Table: Energy, nutrient and phytochemical‐rich foods intake across quartiles of the DPI in case and control groups.
Logistic regression results are shown in Table4. In the crude model, higher DPI was associated with a reduced odds of DOR (Q4 vs. Q1 OR: 0.79; 95% CI: 0.55–0.93;p‐trend = 0.01). After adjustment for physical activity and energy intake (Model 1), the association remained significant (OR: 0.80; 95% CI: 0.54–0.95;p‐trend = 0.033). In the fully adjusted model (Model 2), women in the highest DPI quartile had 27% lower odds of DOR compared to those in the lowest quartile (OR: 0.73; 95% CI: 0.42–0.97;p‐trend = 0.02).
Table: Crude and adjusted associations between DPI scores and the odds of DOR among the study population.
Discussion
This study is, to our knowledge, the first to explore the relationship between the DPI and DOR in women of reproductive age. Our findings suggest that individuals with higher DPI scores, reflecting greater intake of phytochemical‐rich foods, had significantly lower odds of experiencing DOR. In particular, women in the highest DPI quartile had 27% lower odds of DOR compared to those in the lowest quartile, even after accounting for potential confounding factors such as physical activity, energy intake, BMI, and fat mass. These findings indicate that diets rich in phytochemicals may exert a protective effect against ovarian aging and support reproductive health. Moreover, among the control group, significant variation in AFC was observed across DPI quartiles, further supporting the link between dietary quality and ovarian reserve.
DOR, defined by a decline in both the number and quality of oocytes, may result in early onset of menopause and reduced fertility potential [26]. This decline typically represents a physiological consequence of advancing age, occurring in the absence of underlying pathological conditions [26]. However, the variable rate of ovarian reserve decline among reproductive‐aged women suggests influences beyond age [2]. Although the exact aetiology of DOR is not fully understood, several factors have been implicated, including ovarian surgery, exposure to gonadotoxic treatments, genetic predispositions, autoimmune disorders, and various environmental or lifestyle factors such as smoking, inadequate nutrition, and chronic psychological stress [2,27]. Despite the lack of comprehensive studies examining the specific effects of diet on ovarian reserve, available evidence suggests that vegetarian and plant‐based diets, which are rich in dietary phytochemicals, may exert beneficial effects on female fertility [28].
Phytochemicals are generally characterised as bioactive, non‐nutritive compounds synthesised as secondary metabolites in plants, predominantly produced as a defence mechanism against environmental stressors, and are widely distributed in fruits, vegetables, whole grains, nuts, and other plant‐derived foods [10]. Key dietary phytochemicals include polyphenols, carotenoids, isoprenoids, phytosterols, saponins, organosulfur compounds, and dietary fibres [10]. These compounds have been shown to confer protective effects against a range of metabolic disorders, including insulin resistance, impaired glucose metabolism, and lipid dysregulation, primarily through their anti‐inflammatory actions and antioxidant properties [29]. In this context, the DPI has been introduced as a novel dietary tool to assess the associations between the consumption of phytochemical‐rich foods and various health outcomes in epidemiologic studies [24].
As this is, to the best of our knowledge, the first study to examine the association between the DPI and DOR, opportunities for direct comparison with previous research are limited. Nonetheless, there is emerging evidence suggesting beneficial effects of adherence to the DPI, as a measure of phytochemical intake, on reproductive disorders such as PCOS [11,17]. For instance, Chi et al. reported a reverse association between higher adherence to DPI and unfavourable metabolic and hormonal profiles in women with PCOS [17]. Besides, a recent scoping review encompassing 18 clinical trials highlighted the beneficial effects of phytochemical‐rich supplements and diets, which exert antioxidant and anti‐inflammatory properties, leading to improvements in hormonal and metabolic markers among women with PCOS [11], further supporting the potential role of phytochemical intake in reproductive health management. Additionally, both experimental and clinical studies suggest that specific phytochemicals, such as phytoestrogens, flavonoids, and certain herbal extracts, can modulate key reproductive hormones, including LH, FSH, prolactin, oestrogen, and progesterone, particularly in conditions like PCOS and hypogonadism [30,31]. More specifically, findings from other animal models have demonstrated that various phytochemicals enhance ovarian reserve indicators, particularly AMH levels, suggesting their potential role in preserving follicular function and reproductive capacity [32].
Although human trials on the effects of phytochemicals on ovarian reserve are still lacking, highlighting a key gap in fertility research, several studies have shown that the DPI is inversely associated with a range of health conditions such as metabolic syndrome [33], obesity [34], cancer [35], and chronic kidney disease progression [36]. Notably, in the current study, individuals with higher DPI scores had significantly greater intakes of phytochemical‐rich foods including fruits, vegetables, legumes, whole grains, soy, and tea, further supporting the index's relevance as a marker of health‐promoting dietary patterns and suggesting a potential association underlying our findings. In line with this, previous research has shown that lower fruit intake is associated with prolonged time to pregnancy and an elevated risk of infertility [37]. Accordingly, the Mediterranean Diet, a holistic dietary pattern characterised by high intake of extra virgin olive oil, antioxidant‐ and vitamin‐rich plant foods, whole grains, low‐fat dairy, poultry, and oily fish, has been associated with improved reproductive outcomes. It has been shown that this healthy diet can enhance fertility in both natural conception and assisted reproductive technology (ART) contexts through its anti‐inflammatory and endocrine‐modulating properties [7,8]. Similarly, Kabodmehri et al. recently reported that adherence to an antioxidant‐rich diet, which is comparable to the DPI and highlights the importance of plant‐based foods and overall antioxidant content, may lower the risk of infertility by alleviating oxidative stress and inflammation [38].
Interestingly, in our study, although higher compliance with DPI scores was linked to lower odds of DOR in the overall population, we did not find a significant association between DPI and AMH or AFC levels among women who were already diagnosed with DOR. As a result, this may suggest that the beneficial effects of phytochemical‐rich diets are more relevant to the prevention or slowing of the decline in ovarian reserve, instead of reversing or improving it once DOR has developed. Another possibility is that, in women with DOR, ovarian function may have fallen to a level where dietary influences no longer exert measurable effects on AMH or AFC. Besides, factors that were not accounted for such as the use of drugs with psychological effects, environmental toxins, stress, hormonal or immune‐related disorders [2], and possible reproductive‐specific genetic factors [39] may have contributed to the lack of significant differences observed. It is also worth noting that among the control group, those in the second DPI quartile had the highest AFC levels compared to other categories, suggesting a possible non‐linear association between DPI and ovarian reserve in healthy women. Consequently, greater longitudinal studies are warranted to better understand the timing and nature of the relationship between phytochemical intake and ovarian function throughout the reproductive lifespan.
Although the exact biological mechanisms relating the DPI to ovarian reserve have yet to be understood, extensive evidence suggests that dietary phytochemicals may help reduce inflammation and oxidative stress [13], both of which may play crucial roles in pathogenesis of reproductive abnormalities [40]. Of note, an imbalance in reactive oxygen species (ROS) levels due to oxidative stress could disrupt the critical reproductive processes including oocyte development, follicular progression, luteal phase regulation, and early placental development, ultimately impacting ovarian function and fertility [40,41]. In this regard, accumulated evidence has documented the strong anti‐inflammatory properties of phytochemicals [42]. For example, phytochemical compounds such as resveratrol, quercetin, genistein, kaempferol, and daidzein have been reported to reduce inflammation by suppressing pro‐inflammatory cytokines (e.g., interleukins (IL‐6, IL‐1β), and tumour necrosis factor‐alpha (TNF‐α)) and inhibiting production of nitric oxide through regulation of important signalling pathways like nuclear factor kappa B (NF‐κB) and mitogen‐activated protein kinase (MAPK) [43]. In addition, they have shown to exhibit antioxidant activity by scavenging reactive oxygen and nitrogen species, chelating metal ions, and enhancing the expression of antioxidant enzymes (e.g., catalase, glutathione peroxidase, and superoxide dismutase) [13,43]. Another potential mechanism may be attributed to the beneficial impacts of these compounds on hormonal regulation which is essential for normal reproductive function [44,45]. Nonetheless, despite the proposed mechanisms, investigating underlying biological pathways through inflammatory and oxidative stress biomarkers may shed light on how phytochemical‐rich diets influence reproductive capacity.
A key strength of this study is providing new insights into potentially modifiable risk factors, especially overall diet, that may help prevent or manage DOR. Other advantages include matching groups by age and BMI, a large sample size, and accounting for various possible confounders in the analysis. However, this study has several limitations that should be acknowledged. First, causal relationships cannot be established due to the study's retrospective design. Second, the method used to assess DPI is based on the caloric intake of phytochemical‐rich foods, which means it does not accurately reflect total phytochemical intake, as it excludes non‐caloric but phytochemical‐dense items such as spices, green tea, and black tea. Furthermore, this method does not capture the type and quality of phytochemicals consumed. Third, the lack of a region‐specific food composition database for plant‐based nutrients further restricts the precision and generalizability of DPI estimation since phytochemical profiles can vary considerably across regions. Forth, although we adjusted for major confounders, we could not include all possible confounding variables in the statistical models, as adding additional covariates could reduce statistical power. Therefore, the potential influence of unmeasured factors such as psychological stress, environmental toxins, genetic background, endocrine‐related disorders, occupation, or additional lifestyle variables may have affected the validity of the observed association. Fifth, as this study included women seeking care at fertility clinics, our findings may not be generalizable to the general population. This recruitment strategy may introduce selection bias, as women attending fertility clinics could differ in reproductive characteristics from women in the broader community.
In conclusion, the results of our study suggest that adherence to a high phytochemical diet may reduce the chance of having DOR, supporting the significance of the contribution of dietary factors in the prevention and management of reproductive disorders. Whilst further research, particularly of prospective trials, is needed to confirm the present findings. Moreover, to better understand how dietary phytochemical patterns affect ovarian potential, it is essential to elucidate the underlying mechanisms by measurement of inflammatory and oxidative stress markers.
Author Contributions
Abed Ghavami, Gholamreza Askari and Hatav Ghasemi‐Tehrani; conception and design of the work, Hatav Ghasemi‐Tehrani and Maryam Kalatehjari; study gynecologists, Abed Ghavami, Mahdi Vajdi, Amin Mokari‐Yamchi; analysis and interpretation of data, Maryam Kalatehjari, Abed Ghavami, draft the work and revise it.
Funding
The present study was supported by a grant from Vice‐Chancellor for Research, Isfahan University of Medical Sciences (Grant No: 2401257).
Ethics Statement
Written informed consent was obtained from all participants, and the study followed the principles of the Declaration of Helsinki. Ethical approval was obtained from the Ethics Committee of Isfahan University of Medical Sciences (IR.ARI.MUI.REC.1401.297) with support from the Department of Nutrition, Faculty of Medicine.
Consent
Written informed consent was obtained from all participants.
Conflicts of Interest
The authors declare no conflicts interest.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Associated Data
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
References
- Cedars M. I., “Evaluation of Female Fertility—AMH and Ovarian Reserve Testing,” Journal of Clinical Endocrinology & Metabolism 107, no. 6 (2022): 1510–1519. doi.org/10.1210/clinem/dgac039
- Zhu Q., Li Y., Ma J., Ma H., and Liang X., “Potential Factors Result in Diminished Ovarian Reserve: A Comprehensive Review,” Journal of Ovarian Research 16, no. 1 (2023): 208. doi.org/10.1186/s13048-023-01296-x
- Liu Y., Pan Z., Wu Y., Song J., and Chen J., “Comparison of Anti‐Müllerian Hormone and Antral Follicle Count in the Prediction of Ovarian Response: A Systematic Review and Meta‐Analysis,” Journal of Ovarian Research 16, no. 1 (2023): 117. doi.org/10.1186/s13048-023-01202-5
- Amanvermez R. and Tosun M., “An Update on Ovarian Aging and Ovarian Reserve Tests,” International Journal of Fertility & Sterility 9, no. 4 (2016): 411–415. doi.org/10.22074/ijfs.2015.4591
- Broekmans F. J., Soules M. R., and Fauser B. C., “Ovarian Aging: Mechanisms and Clinical Consequences,” Endocrine Reviews 30, no. 5 (2009): 465–493. doi.org/10.1210/er.2009-0006
- Gaskins A. J. and Chavarro J. E., “Diet and Fertility: A Review,” American Journal of Obstetrics and Gynecology 218, no. 4 (2018): 379–389. doi.org/10.1016/j.ajog.2017.08.010
- Karayiannis D., Kontogianni M. D., Mendorou C., Mastrominas M., and Yiannakouris N., “Adherence to the Mediterranean Diet and IVF Success Rate Among Non‐Obese Women Attempting Fertility,” Human Reproduction 33, no. 3 (2018): 494–502. doi.org/10.1093/humrep/dey003
- Vujkovic M., de Vries J. H., Lindemans J., et al., “The Preconception Mediterranean Dietary Pattern in Couples Undergoing in Vitro Fertilization/Intracytoplasmic Sperm Injection Treatment Increases the Chance of Pregnancy,” Fertility and Sterility 94, no. 6 (2010): 2096–2101. doi.org/10.1016/j.fertnstert.2009.12.079
- Carlos S., De La Fuente‐Arrillaga C., Bes‐Rastrollo M., et al., “Mediterranean Diet and Health Outcomes in the SUN Cohort,” Nutrients 10, no. 4 (2018): 439. doi.org/10.3390/nu10040439
- Kumar A., Nirmal P., Kumar M., et al., “Major Phytochemicals: Recent Advances in Health Benefits and Extraction Method,” Molecules 28, no. 2 (2023): 887. doi.org/10.3390/molecules28020887
- Chavez G. N., Jaworsky K., and Basu A., “The Effects of Plant‐Derived Phytochemical Compounds and Phytochemical‐Rich Diets on Females With Polycystic Ovarian Syndrome: A Scoping Review of Clinical Trials,” International Journal of Environmental Research and Public Health 20, no. 15 (2023): 6534. doi.org/10.3390/ijerph20156534
- Cederroth C. R., Zimmermann C., and Nef S., “Soy, Phytoestrogens and Their Impact on Reproductive Health,” Molecular and Cellular Endocrinology 355, no. 2 (2012): 192–200. doi.org/10.1016/j.mce.2011.05.049
- Chorosho S. H., Malik N., Panesar G., et al., “Phytochemicals: Alternative for Infertility Treatment and Associated Conditions,” Oxidative Medicine and Cellular Longevity 2023 (2023): 1327562. doi.org/10.1155/2023/1327562
- Rais J., Jafri A., Siddiqui S., Tripathi M., and Arshad M., “Phytochemicals in the Treatment of Ovarian Cancer,” Frontiers in Bioscience (Elite Edition) 9, no. 1 (2017): 67–75. doi.org/10.2741/e786
- Qorbani M., Angoorani P., and Ejtahed H.‐S., “Dietary Phytochemical Index as a Biomarker in Nutritional Studies: Features and Applications,” in Biomarkers in Nutrition, ed. Patel V. B. and Preedy V. R. (Springer International Publishing, 2022), 1–22.
- Amirkhizi F., Taghizadeh M., Hamedi‐Shahraki S., and Asghari S., “Association of Dietary Phytochemical Index With Metabolic Markers, Serum Asymmetric Dimethylarginine and Atherogenic Indices in Patients With Polycystic Ovary Syndrome,” Nutrition & Metabolism (London) 22, no. 1 (2025): 39. doi.org/10.1186/s12986-025-00932-1
- Chi Y., Yue R., Lv Y., Li H., and Liao W., “The Dietary Phytochemical Index and Its Relation to Polycystic Ovary Syndrome: A Case‐Control Study,” Journal of Ovarian Research 17, no. 1 (2024): 228. doi.org/10.1186/s13048-024-01540-y
- Medicine PCotASfR , “Testing and Interpreting Measures of Ovarian Reserve: A Committee Opinion,” Fertility and Sterility 114, no. 6 (2020): 1151–1157. doi.org/10.1016/j.fertnstert.2020.09.134
- Pastore L. M., Christianson M. S., Stelling J., Kearns W. G., and Segars J. H., “Reproductive Ovarian Testing and the Alphabet Soup of Diagnoses: DOR, POI, POF, POR, and FOR,” Journal of Assisted Reproduction and Genetics 35, no. 1 (2018): 17–23. doi.org/10.1007/s10815-017-1058-4
- Choi R., Park W., Chun G., Lee S. G., and Lee E. H., “Investigation of the Prevalence of Diminished Ovarian Reserve in Korean Women of Reproductive Age,” Journal of Clinical Medicine 12, no. 15 (2023): 5099. doi.org/10.3390/jcm12155099
- Nikniaz L., Tabrizi J., Sadeghi‐Bazargani H., Farahbakhsh M., Tahmasebi S., and Noroozi S., “Reliability and Relative Validity of Short‐Food Frequency Questionnaire,” British Food Journal 119, no. 6 (2017): 1337–1348.
- Ghafarpour M., Houshiar‐Rad A., and Kianfar H., The Manual for Household Measures, Cooking Yields Factors and Edible Portion of Foods, vol. 7 (Nashre Olume Keshavarzy, 1999), 42–58.
- Azar M. and Sarkisian E., Food Composition Table of Iran: National Nutrition and Food Research Institute (Shaheed Beheshti University, 1980).
- McCarty M. F., “Proposal for a Dietary “Phytochemical Index”,” Medical Hypotheses 63, no. 5 (2004): 813–817. doi.org/10.1016/j.mehy.2002.11.004
- Moghaddam M. B., Aghdam F. B., Jafarabadi M. A., Allahverdipour H., Nikookheslat S. D., and Safarpour S., “The Iranian Version of International Physical Activity Questionnaire (IPAQ) in Iran: Content and Construct Validity, Factor Structure, Internal Consistency and Stability,” World Applied Sciences Journal 18, no. 8 (2012): 1073–1080.
- “Testing and Interpreting Measures of Ovarian Reserve: A Committee Opinion,” Fertility and Sterility 103, no. 3 (2015): e9–e17. doi.org/10.1016/j.fertnstert.2014.12.093
- Yan F., Zhao Q., Li Y., et al., “The Role of Oxidative Stress in Ovarian Aging: A Review,” Journal of Ovarian Research 15, no. 1 (2022): 100. doi.org/10.1186/s13048-022-01032-x
- Cristodoro M., Zambella E., Fietta I., Inversetti A., and Di Simone N., “Dietary Patterns and Fertility,” Biology‐Basel 13, no. 2 (2024): 131. doi.org/10.3390/biology13020131
- Martín M. Á. and Ramos S., “Effects of Phytochemicals on Metabolic Diseases and Human Health,” Nutrients 16, no. 24 (2024): 4323. doi.org/10.3390/nu16244323
- van Die M. D., Burger H. G., Teede H. J., and Bone K. M., “Vitex Agnus‐CastusExtracts for Female Reproductive Disorders: A Systematic Review of Clinical Trials,” Planta Medica 79, no. 7 (2013): 562–575. doi.org/10.1055/s-0032-1327831
- Banaszewska B., Wrotyńska‐Barczyńska J., Spaczynski R. Z., Pawelczyk L., and Duleba A. J., “Effects of Resveratrol on Polycystic Ovary Syndrome: A Double‐Blind, Randomized, Placebo‐Controlled Trial,” Journal of Clinical Endocrinology and Metabolism 101, no. 11 (2016): 4322–4328. doi.org/10.1210/jc.2016-1858
- Gökçek İ., Uyanık G., Tutar T., and Gözer A., “Effects of Carvacrol on Hormonal, Inflammatory, Antioxidant Changes, and Ovarian Reserve in Polycystic Ovary Syndrome in Wistar Rats,” Naunyn‐Schmiedeberg's Archives of Pharmacology 398, no. 4 (2025): 4607–4616. doi.org/10.1007/s00210-024-03588-5
- Mehranfar S., Jalilpiran Y., Ejtahed H. S., et al., “Association of Dietary Phytochemical Index With Cardiometabolic Risk Factors,” International Journal for Vitamin and Nutrition Research 93, no. 6 (2023): 559–576. doi.org/10.1024/0300-9831/a000763
- Wei C., Liu L., Liu R., Dai W., Cui W., and Li D., “Association Between the Phytochemical Index and Overweight/Obesity: A Meta‐Analysis,” Nutrients 14, no. 7 (2022): 1429. doi.org/10.3390/nu14071429
- Ahmadirad H., Omrani M., Azmi N., et al., “Dietary Phytochemical Index and the Risk of Cancer: A Systematic Review and Meta‐Analysis,” PLoS One 20, no. 4 (2025): e0319591. doi.org/10.1371/journal.pone.0319591
- Bahrampour N., Mirzababaei A., Hosseininasab D., Abaj F., Clark C. C. T., and Mirzaei K., “High Intake of Dietary Phytochemical Index May Be Related to Reducing Risk of Diabetic Nephropathy: A Case–Control Study,” BMC Nutrition 9, no. 1 (2023): 14. doi.org/10.1186/s40795-023-00676-2
- Alesi S., Habibi N., Silva T. R., et al., “Assessing the Influence of Preconception Diet on Female Fertility: A Systematic Scoping Review of Observational Studies,” Human Reproduction Update 29, no. 6 (2023): 811–828. doi.org/10.1093/humupd/dmad018
- Kabodmehri R., Javaheri F. S. H., Alami F., et al., “Female Infertility and Dietary Antioxidant Index (DAI); a Case‐Control Study,” BMC Women's Health 23, no. 1 (2023): 608. doi.org/10.1186/s12905-023-02747-9
- Moiseeva A. V., Kudryavtseva V. A., Nikolenko V. N., et al., “Genetic Determination of the Ovarian Reserve: A Literature Review,” Journal of Ovarian Research 14, no. 1 (2021): 102. doi.org/10.1186/s13048-021-00850-9
- Agarwal A., Gupta S., and Sharma R. K., “Role of Oxidative Stress in Female Reproduction,” Reproductive Biology and Endocrinology 3, no. 1 (2005): 28. doi.org/10.1186/1477-7827-3-28
- Moustakli E., Stavros S., Katopodis P., et al., “Oxidative Stress and the NLRP3 Inflammasome: Focus on Female Fertility and Reproductive Health,” Cells 14, no. 1 (2025): 36. doi.org/10.3390/cells14010036
- Pan M. H., Lai C. S., and Ho C. T., “Anti‐Inflammatory Activity of Natural Dietary Flavonoids,” Food & Function 1, no. 1 (2010): 15–31. doi.org/10.1039/c0fo00103a
- Upadhyay S. and Dixit M., “Role of Polyphenols and Other Phytochemicals on Molecular Signaling,” Oxidative Medicine and Cellular Longevity 2015 (2015): 504253. doi.org/10.1155/2015/504253
- Cojocneanu Petric R., Braicu C., Raduly L., et al., “Phytochemicals Modulate Carcinogenic Signaling Pathways in Breast and Hormone‐Related Cancers,” Oncotargets and Therapy 8 (2015): 2053–2066. doi.org/10.2147/OTT.S83597
- Domínguez‐López I., Yago‐Aragón M., Salas‐Huetos A., Tresserra‐Rimbau A., and Hurtado‐Barroso S., “Effects of Dietary Phytoestrogens on Hormones Throughout a Human Lifespan: A Review,” Nutrients 12, no. 8 (2020): 2456. doi.org/10.3390/nu12082456
Republished from the open web under CC-BY. Authors: Khodarahmi M, Askari G, Vajdi M, Mokari-Yamchi A, Ghasemi-Tehrani H, Kalatehjari M, Ghavami A. Read the original.