Effectiveness of Alcohol Use Disorder Pharmacotherapies by Sex: Systematic Review and Meta-Analysis.
Issues Alcohol use disorder (AUD) shows sex-related differences in prevalence, harm and treatment response. Despite growing interest in sex differences, evidence synthesis evaluating pharmacotherapy effectiveness by sex remains limited. Approach Web of Science, PubMed, Scopus, PsycINFO and Cochrane were searched twice. Eligible records included RCTs or non-randomised studies of adults with AUD receiving pharmacological interventions (licensed or off-label), and reporting or providing outcomes (binary relapse or continuous alcohol consumption change) by sex. Multi-level random-effects models calculated risk ratios (RR) and standardised mean differences (SMD), with sex as a moderator. Key findings Twenty-eight studies (25,041 participants, 25% female) were included. No outcomes were rated low risk of bias; non-RCTs were moderate-to-high quality. Overall treatment effects vs. control were small for abstinence (RR = 0.96, 95% CI [0.52, 1.74]; 4 studies; I 2 = 95%) and modest for consumption reduction (SMD = 0.23, 95% CI [0.01, 0.45]; 13 studies; I 2 = 89%); sex did not meaningfully moderate these outcomes (ratio of RR = 1.04, 95% CI [0.87, 1.25]; ΔSMD = 0.05, 95% CI [-0.09, 0.18]). Power was low (median 13.7%), requiring ~6358 participants per group to detect the observed sex difference. Narrative synthesis suggested possible sex differences for naltrexone and baclofen, while highlighting the influence of drug (e.g., tolerability), participant (e.g., drinking motives) and design factors (e.g., recruitment setting) on treatment response. Implications AUD pharmacotherapies provide modest benefits, with sex differences remaining unclear. Future trials should be adequately powered, report sex-specific outcomes and consider adherence, tolerability and psychosocial moderators. Conclusion Evidence for sex-specific efficacy remains inconclusive. Patterns for naltrexone and baclofen warrant exploration in large, rigorously designed, sex-stratified trials.
Introduction
Alcohol use disorder (AUD) is characterised by impaired control over alcohol consumption despite adverse consequences [1]. While overall consumption is declining across Europe [2], the impact of alcohol on health is rising [3,4,5]. In the United Kingdom (UK), alcohol‐specific deaths reached a record high in 2023, while alcohol‐related mortality increased by 39% in women and 38% in men between 2019 and 2023 [6,7]. Similarly, from 1999 to 2020, the United States of America (USA) saw a 14.7% rise in alcohol‐related mortality for women and 12.5% for men [8].
Men typically consume more alcohol [2], leading to higher rates of alcohol‐related hospitalisations and fatalities [9,10,11]. However, women tend to be more vulnerable to the harmful effects of alcohol, even at lower consumption levels [12,13]; they face increased risk of developing severe alcohol‐related liver disease, certain cancers, and cardiovascular disease despite lower alcohol intake [11,14,15]. National Survey on Drug Use and Health data (2009–2019) show that although overall AUD rates declined, this decline was significantly steeper among men than women [16]. Across health‐related pre‐clinical and clinical research, female animals and participants have historically been underrepresented due to concerns that hormonal fluctuations would introduce variability into the data [17,18]. However, there is a rising demand for research to inform targeted treatments and support for women's alcohol use [19,20].
Several mechanisms may underlie differences in pharmacotherapy effectiveness by sex. For example, female sex hormones (oestrogen and progesterone) can influence sensitivity to opioid antagonists with women experiencing differential subjective effects across their menstrual cycle [21,22]. Sex differences in pharmacokinetics influence variations in peak drug concentration and bioavailability affecting the levels and duration of action of medications [23,24]. A recent review found poorer tolerability and more severe side effects from acamprosate, naltrexone, baclofen and varenicline in women, potentially affecting adherence [25]. Gender‐related factors, such as differences in stress‐related drinking [26,27] and early evidence suggesting that anxiolytic medications may be more effective in women [28], could impact treatment outcomes.
Despite these observations, literature on sex differences in AUD treatment response is limited and requires synthesis [29,30] This systematic review and meta‐analysis aim to: (i) determine whether the effectiveness of AUD pharmacotherapies differs by sex; and (ii) identify whether mechanisms of therapeutic effect differ by sex.
Methods
Protocol and Registration
The review protocol was registered with the International Prospective Register of Systematic Reviews (PROSPERO) ID: CRD42023372885. The review adheres to the 2020 Preferred Reporting Items for Systematic Reviews and Meta‐analyses [31], as detailed in TableS3. Web of Science, PubMed, Scopus, PsycINFO and Cochrane were searched in May 2023 and updated in January 2025. The search strategy combined AUD population, pharmacological intervention, and treatment status terms; ‘AND’ was used to combine the three searches and identify relevant studies (TableS1). Sex and gender terms were not included in the search strategy to maximise study inclusion, as some trials report outcomes by sex/gender without indexing. Full texts were briefly assessed during early screening for sex‐disaggregated outcomes. This review uses the term ‘sex’ when discussing differences in pharmacotherapy response. Accordingly, the termsfemaleandmaleare used as adjectives to describe trial participants throughout the results. However, gender, encompassing social, psychological and behavioural factors can influence treatment outcomes [32,33]. Where appropriate, particularly when referring to population‐level trends or gendered experiences, the termswomenandmenare used as nouns.
Study Selection and Eligibility Criteria
Study selection and eligibility criteria targeted English‐language studies reporting AUD treatment outcomes by sex. Eligible studies included randomised controlled trials (RCT) and non‐randomised studies. Interventions were pharmacotherapies, licensed or unlicensed, for AUD treatment, excluding those used for managing alcohol withdrawal syndrome. A review of the literature and a recent meta‐analysis [34] identified 34 frequently prescribed pharmacotherapies for maintaining abstinence in AUD patients. Inclusion required baseline and/or post‐treatment alcohol use outcomes, such as changes in alcohol consumption quantity or frequency (Table1).
Table: Eligibility criteria for study selection.
Data requests were made to authors of studies lacking sex‐disaggregated outcomes, covering 247 reports across 154 corresponding authors. Contact could not be established for 16% of authors, often due to unavailable or undeliverable e‐mail addresses, particularly for older publications; 47% did not respond, 19% indicated that the data were no longer accessible, 4% declined to share data and 8% provided additional data (Figure1).
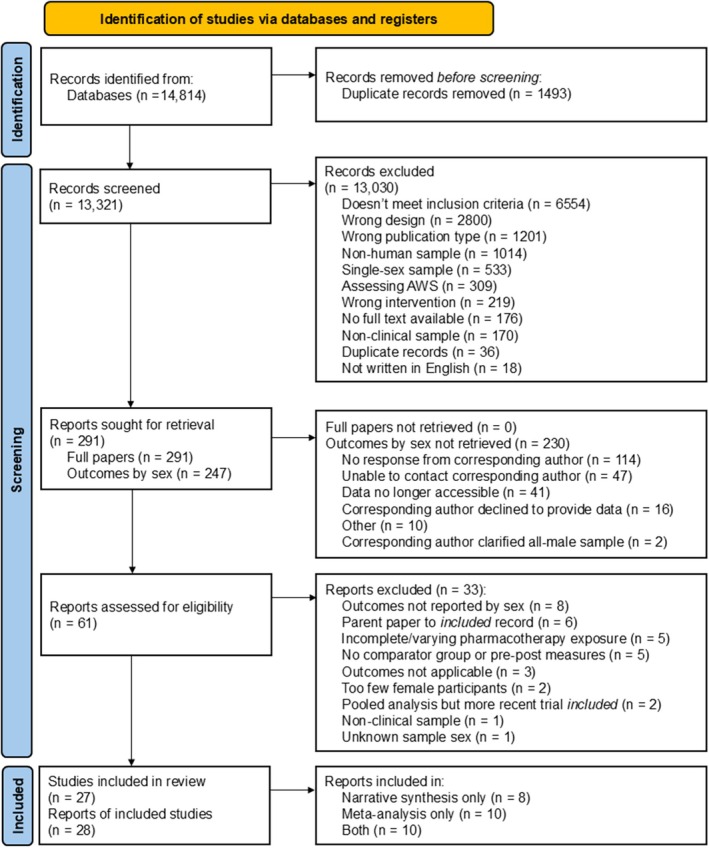
Preferred reporting items for systematic reviews and meta‐analyses (PRISMA) flow chart. The figure presents the PRISMA flow diagram detailing study identification, screening, eligibility assessment and final inclusion in the current systematic review and meta‐analysis. The initial database search yielded 14,814 records. After the removal of 1493 duplicates, 13,321 citations were eligible for title and abstract screening. This first phase of screening excluded of 13,030 records for various reasons: 6554 did not meet the main inclusion criteria 2800 used the wrong study design, 1201 were the wrong publication type, 1014 were not on human samples, 533 examined single‐sex samples, 309 assessed alcohol withdrawal syndrome (AWS), 219 concerned the wrong intervention, 176 lacked available full texts, 170 were on non‐clinical samples, 36 were newly identified duplicates, and 18 were not written in English. Following this, 291 reports were sought for retrieval for full‐text screening, comprising 44 readily available full texts and 247 reports for which the authors were contacted to provide sex‐specific outcome data. The second phase of screening excluded 33 reports for reasons including: Failure to report required outcomes by sex (n= 8), being a parent paper to an already included record (n= 6), having incomplete or varying pharmacotheraphy exposure (n= 5), reporting only non‐applicable outcomes (n= 3), having too few female participants (n= 2), being an older pooled analysis of an included record (n= 1), being on a non‐clinical sample (n= 1) and having unknown sample sex (n= 1). Ultimately, 28 records, representing 27 unique studies, were included in the review. Of these, 8 records were included in the narrative synthesis only, 10 were included in the meta‐analysis only and 10 were included in both.
All titles and abstracts were screened by two independent reviewers with overall agreement of 95.12%. Full‐text papers were obtained and independently screened for final inclusion, with an agreement rate of 80.44%. Studies excluded at the full‐text screening stage are detailed in TableS5.
Data Extraction
The following data were extracted: author, publication date, journal, country, publication type, funding source, reported conflict(s) of interest, study design, inclusion and exclusion criteria, study setting, use of ‘sex’ or ‘gender’, sample co‐morbidities, AUD assessment method, participant drinking status at baseline, alcohol‐related measures and outcomes, secondary measures and outcomes, number of data collection points, attrition, intervention details and alcohol use outcomes at baseline and follow‐up. Where data were only included in graphs/figures, values were estimated using Webplot Digitizer 3.1 (http://arohatgi.info/WebPlotDigitizer). See TableS2for all required data conversions.
Risk of Bias
For outcomes derived from RCTs, the Cochrane Risk of Bias (RoB) 2 tool was employed to assess quality [35]. The JBI Critical Appraisal Tool was used for non‐randomised studies, evaluating criteria pertinent to cohort designs [36]. Each study was assessed independently by two reviewers using standardised templates. Once independent evaluations were complete, reviewers discussed any discrepancies (agreement rate: 73%). Industry sponsorship was identified in 48.28% of reports, primarily through medication donations (64%), unspecified support (21%), or direct monetary contributions (14%). Seven reports were flagged as high risk of bias due to disclosed conflicts of interest or insufficient transparency. High risk of bias, determined by RoB 2, the JBI, and conflicts of interest, was factored into analyses. GRADE assessments [37] were carried out for the three primary outcomes (binary results, between‐subject continuous outcomes [treatment vs. control] within‐subject continuous outcomes).
Narrative Synthesis
Narrative synthesis was conducted following Popay et al. [38]. The initial stage involved data visualisation (FigureS5). The visualised data facilitated a preliminary synthesis of the findings, helping to organise the results and identify patterns across studies regarding the direction and magnitude of effects while also beginning to explore influential factors. Descriptive summaries of each study were drafted within the categories of pharmacotherapy and mechanism of action.
Meta‐Analytic Approach
All meta‐analyses were conducted in R (version 2024.12.0) using the ‘metafor’, ‘dmetar’ and ‘dplyr’ packages. Multi‐level random‐effects models were used to account for the nested data structure, where multiple effect sizes were drawn from the same study. Outcomes were coded so that larger effect sizes consistently indicated a positive treatment response (e.g., greater abstinence or reduced consumption). Outcomes where higher values reflected poorer responses (e.g., relapse or greater drinking days) were reverse coded before analysis.
Between‐subject effects were calculated using Cohen'sdas the effect size metric (standardised mean difference; SMD). Two between‐subject models were examined: one including all comparisons (e.g., treatment vs. another drug or control), and a restricted model including only comparisons against true control conditions (placebo, treatment as usual or no treatment) to enhance interpretability. Within‐subject effects were calculated as standardised mean change scores (SMCC) using raw score standardisation. A pre–post correlation of 0.7 was conservatively imputed for SMCC calculations. Binary outcomes (e.g., abstinence, relapse) were analysed using log‐transformed risk ratios (logRR). All models were conducted on the log scale, and final estimates were exponentiated for interpretability. Effect sizes were interpreted using conventional benchmarks: 0.2 (small), 0.5 (moderate), and 0.8 (large) for both SMD and SMCC. Risk ratios were interpreted on the log scale, with values of 1.0 indicating no effect.
Subgroup analyses and meta‐regression models were conducted to explore whether treatment effects differed by, or interacted with, treatment class, region, baseline drinking status, treatment duration (categorised as ≤ 12 weeks or > 12 weeks), presence of psychiatric comorbidities, and RoB. Continuous moderators included treatment duration, sample mean age, and baseline alcohol consumption. As pre‐specified in the PROSPERO protocol, subgroup analyses were conducted only where four or more independent trials were available, and meta‐regressions were conducted only where 10 or more independent trials were available [39].
Heterogeneity was assessed usingI2statistics derived from multilevel variance components [40]. Publication bias was examined through funnel plots and Egger's regression test. As Egger's test cannot be applied to multi‐level models, single‐level models (rma.uni) were also conducted. Statistical power was evaluated for each effect size using the standard error derived from the reported sampling variance and the pooled effect size estimate obtained from the treatment vs. control meta‐analysis. Minimum per‐group sample sizes required to detect the overall pooled effect and the observed sex‐by‐treatment interaction were estimated using the ‘pwr.t.test’ function from the ‘pwr’ package. All primary analyses, including domain‐level models, subgroup, and moderator analyses were pre‐specified and registered on PROSPERO. Full analytic code is available inSupporting Information.
Results
Study Characteristics
The searches yielded 14,814 citations, of which 28 met inclusion criteria (Figure1). Of 27 unique studies, a total of 25,041 participants were included; 6316 were female (25% of the sample) and 18,647 were male. Sample sizes varied between 12 and 14,697 participants, with a mean of 927 (±2984). The percentage of female participants in the trials ranged from 3% to 59%, with a mean of 32.11% (±12.44). Most reports primarily used only the term ‘sex’ (n= 12), while 8 used only ‘gender’; 6 reports employed both terms interchangeably, and 2 did not mention either. Only two studies defined how or explicitly addressed whether they were assessing sex differences.
Three reports employed non‐randomised designs [41,42,43] (including secondary analyses of health records and longitudinal studies), and three reports were open‐label trials [44,45,46]. The remaining 22 reports consisted of RCTs (including RCT‐derived data) [47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68]. Naltrexone was the most frequently studied pharmacotherapy (n= 10) [45,46,48,50,53,56,58,63,65,68], followed by baclofen (n= 6) [43,44,54,55,60,64], varenicline (n= 3; two of which were the same trial) [49,51,62] and (es)citalopram (n= 3) [47,67,69]. Only one report each evaluated acamprosate [59], nalmefene [57], flupenthixol [66] and levetiracetam [52], while two studies compared multiple interventions [41,42] (see Table2).
Table: Study characteristics of included reports (ordered by pharmacotherapy and date).
Binary outcomes includedAbstinence Rate,Relapse RateandNo Heavy Drinking Days Rate. Continuous outcomes included both consumption frequency related measures: Count/Percent/Event Rate ofDrinking Days,Heavy Drinking Days,Abstinent DaysandNon‐Heavy Drinking Days; and consumption quantity related measures:Drinks per Drinking Day,Drinks per DayandTotal Drinks.
Risk of Bias
Forty‐seven outcomes across 22 RCTs were assessed for risk of bias (see FigureS1). Overall, 55.3% of outcomes were rated as having some concerns, with the remaining 44.7% rated as high risk of bias. Outcome measurement was the most robust domain (95.7% low risk), reflecting consistent use of validated tools and appropriate blinding. The most problematic domain was the selection of reported results (91.5% some concern/high risk), stemming from post hoc analyses where sex/gender was explored without clearly pre‐specified outcomes. Five non‐RCTs were assessed using the JBI checklist and scores ranged from moderate to high, with individual scores between 54.6% and 81.8%. All studies measured exposures consistently across groups and reported sufficient follow‐up periods. However, only 40% adequately addressed attrition and described attrition‐management strategies.
Meta‐Analysis
Primary Analyses
There were small but positive treatment effects for overall efficacy measures, see Table3for full results. Positive effect sizes reflect beneficial treatment responses (i.e., reduced consumption or increased abstinence). Male participants were the reference group in all sex‐moderator analyses; positive moderator estimates for continuous outcomes or ratios of relative risks ≥ 1 for binary outcomes indicate greater treatment effects in male participants.
Table: Main treatment effect, pooled estimates by sex and sex moderation effect by multi‐level meta‐analysis of pharmacotherapy effectiveness.
Inspection of forest plots revealed that all confidence intervals (CI) overlapped, so no observations were removed. Heterogeneity was high, withI2ranging from 55.34% to 98.37%. See Figures[Link],[Link]for forest plots.
For binary outcomes (AbstinenceandNo Heavy Drinking Days Rate), the pooled effect comparing treatment to control suggested minimal difference (RR = 0.96,p= 0.88, 95% CI [0.52, 1.74]), with wide confidence intervals encompassing both potential benefit and harm. Sex‐moderator analyses showed similarly imprecise effects, with no meaningful difference between male and female participants (ratio of risk ratio = 1.04,p= 0.66, 95% CI [0.87, 1.25]).
For continuous outcomes (consumption reduction), the pooled effects indicated small beneficial effects: treatment versus control (SMD = 0.23,p= 0.043, 95% CI [0.01, 0.45]), treatment to other drug or control (SMD = 0.22,p= 0.043, 95% CI [0.01, 0.43]), as well as within‐subject change (SMCC = 0.97,p< 0.001, 95% CI [0.54, 1.39]). Sex‐moderator effects were small and imprecise, with confidence intervals including zero: ΔSMD = 0.05,p= 0.51, 95% CI [−0.09, 0.18], treatment versus control; ΔSMD = 0.05,p= 0.17, 95% CI [−0.02, 0.12], treatment versus other drug or control; ΔSMCC = −0.10,p= 0.74, 95% CI [−0.70, 0.50], within‐subject change.
For frequency reduction, the pooled estimated and wide confidence intervals suggested little difference between treatment and control (SMD = 0.23,p= 0.091, 95% CI [−0.04, 0.48]). When adding sex as a moderator, there was no meaningful difference between male and female participants (ΔSMD = 0.05,p= 0.57, 95% CI [−0.11, 0.20]). Similar patterns were observed when comparing treatment to other drug or control and within‐subject change.
For quantity reduction, the pooled effect comparing treatment to other drug or control was small (SMD = 0.24,p= 0.078, 95% CI [−0.03, 0.51]), indicating that the true effect could range from minimal harm to moderate benefit. However, when excluding other drugs in the comparison, the pooled effect remained small, but the confidence interval excluded zero (SMD = 0.25,p= 0.047, 95% CI [0.01, 0.49]), suggesting a small to moderate beneficial effect. Neither of these comparisons was moderated by sex (ΔSMD = 0.08,p= 0.70, 95% CI [−0.33, 0.49], treatment vs. other drug or control; ΔSMD = 0.07,p= 0.71, 95% CI [−0.30, 0.44], treatment vs. control). Within‐subject analyses showed a positive treatment effect (SMCC = 1.14,p< 0.001, 95% CI [0.83, 1.45]), with sex‐moderator estimates close to zero (ΔSMCC = −0.15,p= 0.23, 95% CI [−0.38, 0.09]).
Subgroup Analyses
In line with the registered protocol, a minimum of four studies was required to conduct categorical subgroup analyses, see Table4for full results.
Table: Subgroup main treatment effect, pooled estimates by sex and sex moderation effect by multi‐level meta‐analyses.
In outcomes with low/medium RoB, pooled estimates suggested small beneficial effects on overall efficacy (SMD = 0.18,p= 0.001, 95% CI [0.08, 0.29]) and consumption frequency (SMD = 0.21,p= 0.001, 95% CI [0.09, 0.33]). Sex‐moderator analyses were small and imprecise for overall efficacy (ΔSMD = 0.03,p= 0.79, 95% CI [−0.19, 0.25]), consumption frequency (ΔSMD = 0.11,p= 0.38, 95% CI [−0.14, 0.36]), and consumption quantity (ΔSMD = −0.19,p= 0.33, 95% CI [−0.60, 0.19]).
Compared to control, opioid receptor agonists (naltrexone and nalmefene) demonstrated small but positive treatment effects on overall efficacy (SMD = 0.17,p< 0.001, 95% CI [0.04, 0.30]), consumption frequency (SMD = 0.18,p= 0.001, 95% CI [0.05, 0.31]) and consumption quantity (SMD = 0.20,p= 0.02, 95% CI [0.03, 0.37]). Sex‐moderator analyses were small and imprecise, with confidence intervals including zero for overall efficacy (ΔSMD = 0.09,p= 0.24, 95% CI [−0.06, 0.24]), consumption frequency (ΔSMD = 0.15,p= 0.067, 95% CI [−0.01, 0.31]), and consumption quantity (ΔSMD = −0.31,p= 0.13, 95% CI [−0.70, 0.09]).
For studies conducted in North America, pooled estimates suggested small beneficial effects on overall efficacy (SMD = 0.12,p= 0.040, 95% CI [0.00, 0.24]) and consumption quantity (SMD = 0.17,p= 0.030, 95% CI [0.02, 0.32]). Sex‐moderator analyses were generally imprecise for both overall efficacy (ΔSMD = 0.12,p= 0.08, 95% CI [−0.01, 0.25]) and consumption quantity (ΔSMD = 0.01,p= 0.98, 95% CI [−0.36, 0.37]). For consumption frequency, the main effect was small and imprecise (SMD = 0.13,p= 0.058, 95% CI [−0.01, 0.26]), but the sex‐moderator model suggested an advantage in male participants (ΔSMD = 0.15,p= 0.049, 95% CI [0.01, 0.23]).
All remaining subgroup comparisons showed small or imprecise effects in both the main and sex‐moderated models, with confidence intervals including zero, indicating no clear evidence of subgroup‐specific differences.
Sensitivity Analyses
When the single non‐randomised study was removed, the pooled effect comparing treatment to control remained similar in magnitude, though the CI included zero (SMD = 0.24,p= 0.076, 95% CI [−0.03, 0.51]; 11 trials;I2= 77%) and the sex‐moderator model remained small and imprecise (ΔSMD = 0.11,p= 0.33, 95% CI [−0.11, 0.34]).
For within‐subject change, sufficient data were available to conduct separate analyses for randomised and non‐randomised studies. Among RCTs, the pooled estimate indicated a significant reduction in consumption (SMCC = 1.44,p< 0.001, 95% CI [1.03, 1.85]; 11 trials;I2= 91%) but there was still no meaningful sex moderation (ΔSMCC = −0.14,p= 0.41, 95% CI [−0.49, 0.20]). Similar results were observed for non‐randomised studies, where the pooled effect also showed a significant reduction in consumption (SMCC = 1.20,p< 0.001, 95% CI [0.74, 1.65]; 4 studies;I2= 79%), with no evidence of sex moderation (ΔSMCC = −0.14,p= 0.38, 95% CI [−0.46, 0.18]).
Regression Analyses
Meta‐regression analyses were conducted with each moderator first examined independently, followed by interaction models including sex × moderator terms (TableS4).
Across analyses, baseline severity, sample age, and treatment duration were associated with small effect sizes, and the 95% confidence intervals for all estimates included zero, indicating no clear evidence of meaningful moderation.
Publication Bias
Publication bias is unlikely to have meaningfully influenced the observed treatment effects (see FigureS6for full results, plots and GRADE assessments for the three primary outcomes). Power analyses based on the drug vs. control models for continuous consumption outcomes showed 299 participants (80% power,α= 0.05) per group would be required to detect the observed overall effect (SMD = 0.23); detecting the observed sex difference (ΔSMD = 0.05) would require ~6358 per group. The median observed power across studies was 13.7%.
Narrative Synthesis
GABAergic and Glutamatergic Modulators
Garbutt et al. [54] found no treatment effect or sex interaction at 30 mg ofbaclofenover 12 weeks. In contrast, Garbutt et al. [55] found that baclofen doses (30 and 90 mg groups) reducedHeavy Drinking Daysand increasedAbstinent Dayswith significant sex interactions; female participants receiving 30 mg improved more than those on placebo; this was not observed in males. Morley et al. [60] also reported significantAbstinent Daysincrease in female participants at 30–75 mg doses. Reynaud et al. [64] found no overall treatment effect at 180 mg, though female participants receiving baclofen had significantly higherAbstinence Ratesthan those on placebo. Differences in sample severity and recruitment context may explain this heterogeneity. Garbutt et al. [54] recruited from the community and reported mild baseline severity, whereas Reynaud [64] drew from specialist hospitals. Additionally, adverse event profiles varied by sex. Garbutt et al. [55] found that female participants reported more sedation and fatigue, particularly at higher doses, and were more likely to discontinue treatment. However, no sex differences were found in baclofen concentrations, suggesting the increased sensitivity in female patients may reflect a pharmacodynamic effect.
Fertig et al. [52] evaluatedlevetiracetamin a 10‐week trial and found no significant reductions inHeavy Drinking Daysand no sex‐by‐treatment interaction. Fatigue was the only adverse event more common in the active group; dose or sample characteristics were suggested as possible contributors to the null findings.
Serotonergic and Dopaminergic Modulators
Two trials assessedcitalopram(40 mg daily for 12 weeks). Naranjo et al. [61] recruited a mild/moderate AUD sample, while Adamson et al. [47] studied AUD patients with co‐occurring major depression. Neither trial found significant differences between citalopram and placebo onAbstinent Days, nor significant sex‐by‐treatment interactions. Naranjo et al. [61] found a sex‐specific effect for citalopram when controlling for baseline depression and anxiety. Male participants showed a significantly greater reduction inDrinks per Daythan female participants. However, this finding is complicated by the lack of an effect onDrinks per Drinking Day(a measure that may better capture true drinking quantity by excluding abstinent days). Furthermore, female participants had fewerDrinks per Dayat baseline; this limited scope for improvement may also contribute to the lack of a treatment effect seen in this group.
Wiesbeck et al. [66] conducted a 6‐month RCT comparingflupenthixolto placebo. Flupenthixol was associated with higher relapse rates overall, driven by significantly worse outcomes in male participants. Although female participants on flupenthixol reported fewer relapses than those on placebo, this difference was not statistically significant.
Two trials assessedvarenicline(2 mg daily) in AUD in participants. O'Malley et al. [62] and Bold et al. [49] reported findings from the same 16‐week placebo‐controlled trial and found that varenicline reduced alcohol consumption, but differences from placebo were not statistically significant. A sex‐by‐treatment interaction onHeavy Drinking Daysemerged at 16 weeks, but this interaction was not maintained at the one‐year follow‐up. Male participants reported significantly greaterNo Heavy Drinking Dayscompared to placebo at both end of treatment and one‐year follow‐up, which was not seen in female participants. Female participants were more likely to report adverse events and were less likely to adhere to the medication, which may have contributed to the lack of observed effects. Falk et al. [51] found that varenicline significantly reducedHeavy Drinking Days,Drinks per Dayandper Drinking Daycompared to placebo over 13 weeks, though no sex moderation was observed. That study identified several other potential moderators of treatment response, including age, years of drinking, smoking and treatment goals.
Opioid Receptor Agonists
Hashimoto et al. [57] found thatnalmefene(10–20 mg) significantly reducedHeavy Drinking Dayscompared to placebo. No sex‐by‐treatment interaction was observed. While the authors identified smoking, age and age of AUD onset as significant predictors of treatment response, sex did not moderate outcomes.
Garbutt et al. [53] reported significant reductions inHeavy Drinking Daysin a 380 mg injectablenaltrexonegroup only among male participants. Baros et al. [48] found that 100 mg oral naltrexone significantly increasedAbstinent Daysand reducedHeavy Drinking DaysandDrinks per Drinking Dayfor male, but not female participants. Similarly, Pettinati et al. [63] reported a significant sex‐by‐treatment interaction forAbstinent Ratesamong individuals with co‐occurring CUD; male participants receiving naltrexone were significantly less likely to relapse than placebo, and female participants receiving naltrexone had greater relapse rates than placebo (non‐significant). Tolerability may have influenced outcomes. Garbutt et al. [53] noted that female participants experienced significantly more nausea, particularly at higher doses. Baros et al. [48] also reported greater nausea and sleep disturbances among female participants, and Pettinati et al. [63] observed lower adherence and higher dropout rates among female participants.
Three studies found no evidence of sex differences in naltrexone response. Yoon et al. [45], an 8‐week open‐label study using 50 mg oral naltrexone, observed significant reductions inDrinks per Drinking Dayacross the sample, with no interaction by sex. This study employed split dosing and antiemetic strategies, which may have improved tolerability and limited sex‐related differences. Greenfield et al. [68] examined 100 mg oral naltrexone and found no significant effects onAbstinent Daysor moderation by sex. Goldstein [56] evaluated 380 mg injectable naltrexone in a homeless sample receiving specialist counselling and found positive treatment effects and no sex differences. It may be that specialist intervention attenuated possible sex differences. Limited reporting of side effects and adherence in these studies makes it unclear whether these factors were negligible or simply under‐evaluated.
Discussion
This systematic review and meta‐analysis aimed to evaluate whether the effectiveness of AUD pharmacotherapies varies by sex. Across 25,041 participants, female participants accounted for 25% of the total sample. Overall, pharmacotherapies were associated with modest benefits in reducing alcohol consumption and small effects for abstinence compared with control conditions. The estimated difference in treatment effect between male and female participants was close to zero, and the corresponding confidence intervals were narrow, indicating no clear evidence of a sex‐related difference in treatment response in the available data. Subgroup analyses and the narrative synthesis suggested possible sex differences for naltrexone, baclofen and studies conducted in North America. However, findings were based on limited and heterogeneous data.
Naltrexone was the most frequently studied pharmacotherapy. In the subgroup meta‐analysis of opioid receptor antagonists, moderate overall effects were observed for reducing both frequency and quantity of alcohol consumption, with no clear evidence that these effects differed between male and female participants. The narrative synthesis found that some trials reported greater efficacy in male participants, while others found no sex difference; studies reporting no difference included sample comorbidities, specialist interventions, or strategies to mitigate side effects. These factors are notable, as many studies reported poorer tolerability and higher attrition among female participants. Additionally, naltrexone's efficacy may be moderated by sex and gender related drinking motives. As a μ‐opioid receptor antagonist [70], naltrexone attenuates the positive reinforcing effects of alcohol [71,72], making it particularly effective for individuals driven by reward‐seeking. This aligns with Mann et al. [73], who identified a ‘reward drinker’ phenotype that responded better to naltrexone than placebo. Some evidence suggests men are more likely to consume alcohol/substances for pleasure, reward and enhancement motives [74,75,76]. Studies in the narrative synthesis that found greater efficacy in male participants often included characteristics suggestive of reward sensitivity (e.g., stimulant use, smoking). These traits may reflect a subgroup that aligns more closely with naltrexone's mechanism. However, most studies in the current review did not assess drinking motives or craving profiles, limiting direct evaluation of this hypothesis.
Across several trials, female participants reported higher rates of adverse events, particularly nausea and fatigue, and in some cases showed lower adherence and greater dropout. These differences may be underpinned by sex‐specific pharmacokinetics and hormonal factors. Liu et al. [77] found that women exhibited higher metabolic ratios of 6β‐naltrexol to naltrexone than men, suggesting pharmacokinetic variability. Roche and King [22] further demonstrated that women, particularly during high‐oestrogen phases of the menstrual cycle, show heightened hormonal and subjective responses to naltrexone. Across studies that found no significant sex differences, adverse events and adherence data were rarely disaggregated by sex, limiting further analysis. Further sex‐stratified research evaluating naltrexone response while measuring hormones, tolerability and drinking motives is required.
The narrative synthesis revealed a pattern of greater baclofen efficacy in female participants, which may be related to sex and gender differences in drinking motives and psychiatric profiles. Typically, women are more likely to report drinking in response to stress or negative affect [78,79], while men may be more driven by enhancement or social motives [80,81]. Baclofen, a GABA‐B agonist with anxiolytic properties [82,83], has been shown to be more effective in treating AUD in samples with comorbid anxiety [84]. This aligns with findings from Logge et al. [28], who observed baclofen disrupted the association between stress and drinking in women but not men, suggesting that its anxiolytic effects may be particularly relevant for emotionally motivated drinking. None of the baclofen trials included in the current review stratified drinking motives or baseline anxiety by sex, limiting exploration of this (or other) explanatory mechanisms.
Sex and gender are poorly defined and reported in alcohol treatment research, limiting subgroup analyses and intervention tailoring. A review of 86 youth alcohol studies found that none met the Sex and Gender Equity in Research (SAGER) guidelines [85,86]. In this review, only 2 of 28 trials explained how they conceptualised or assessed sex. Of the 26 reports that used either term, 12 referred only to ‘sex’, 8 only to ‘gender’, and six used terms interchangeably. Studies in this review were selected based on availability of sex‐stratified data reporting, possibly introducing sampling bias, and terminology was assessed without the SAGER framework. However, the findings echo wider evidence that sex and gender are poorly conceptualised and reported in AUD research. There was no reporting of those who are non‐binary, intersex or trans, limiting what we know about their AUD treatment; reporting on these groups would be welcomed [87].
Trial design also limited the investigation of sex differences. Many trials apply exclusion criteria that disproportionately affect women (e.g., pregnancy, breastfeeding or lack of contraception) leading to smaller and more homogeneous female samples that do not represent the diversity of female experience and undermine the generalisability of findings [88]. While intended to minimise risk, these exclusions stem from concerns about reproductive risk, institutional liability, hormonal heterogeneity and assumptions about women's ability to reliably prevent pregnancy [89]. Even when women are included in trials, sex and/or gender are often not meaningfully considered in study design. For example, a common justification for not exploring sex differences in outcomes is the lack of observed differences in baseline characteristics. Yet, standard variables may not capture sex‐ or gender‐sensitive factors influencing treatment outcomes. For example, early substance use, depression, and involvement with child welfare were found to predict poorer outcomes among female participants in outpatient SUD treatment, whereas primary drug use frequency and age at intake were predictive among male participants [90]. Without intentional consideration of sex and gender throughout study design, trials risk overlooking meaningful subgroup differences and mischaracterising treatment effects.
Limitations
Only studies including both male and female participants were eligible. While this allowed for direct sex comparisons under consistent conditions, it excluded female‐ and male‐only trials that may offer valuable insights into pharmacotherapy response. It also excluded trans and gender diverse individuals, on whom we know there are limited studies, despite risk of harm [7]; where possible, studies should avoid reporting as ‘other’ to establish an evidence base [87]. Additionally, the review focused on clinical populations meeting diagnostic criteria for AUD or alcohol dependence. This may limit the applicability of findings to at‐risk populations, where women or other gender representations may be underdiagnosed or underrepresented in treatment settings. Meta‐analyses did not include time‐to‐event outcomes (e.g., time to lapse/relapse), which may be more sensitive to sustained treatment effects.
Recommendations
Research
Future trials must be adequately powered to detect overall effects and sex‐based differences. Exclusion criteria related to reproductive status that disproportionately exclude women should be reconsidered. Trials should predefine sex and/or gender analyses; outcomes related to adherence, side effects, psychosocial variables, drinking motives and treatment goals should all be disaggregated by sex. Variables should include hormonal, reproductive and psychosocial factors; a broader range of baseline variables beyond age and education should be considered. Journals and funders should encourage the use of SAGER guidelines and promote open‐access repositories for sex‐disaggregated data. A consensus core outcome set would improve measurement standards and trial conduct [91,92]. All prescribed AUD medications should be evaluated for sex‐specific efficacy. Large, well‐powered trials should evaluate sex differences in naltrexone and baclofen; naltrexone trials should assess dosing, tolerability, adherence and moderators such as drinking motives and hormonal influences; baclofen trials should consider stress‐ or negative affect–related drinking, baseline anxiety and psychiatric comorbidities.
Practice
Medications like disulfiram, gabapentin, topiramate and antipsychotics lack evidence for women and should not be first‐line treatments. Naltrexone may be more effective in men; for women, consider side effects, anti‐emetics and split dosing. Baclofen may suit women, particularly with stress‐related drinking, but requires careful monitoring. All treatment plans should consider drinking motives, comorbidities and goals.
Conclusions
This review found no consistent evidence that treatment efficacy differs by sex. However, subgroup analyses and narrative findings suggest possible sex‐specific responses in certain contexts, particularly for naltrexone and baclofen. These patterns were more apparent in studies with adequate sex‐stratified analyses. Current evidence is insufficient to support broad conclusions about sex differences in pharmacotherapy response. Nonetheless, the findings highlight the need for adequately powered trials that account for sex‐ and gender‐considered variables. Improving the evidence base requires inclusive research practices, consistent outcome definitions and transparent reporting.
Author Contributions
Each author certifies that their contribution to this work meets the standards of the International Committee of Medical Journal Editors.
Funding
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Associated Data
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- American Psychiatric Association , Diagnostic and Statistical Manual of Mental Disorders [Internet], 5th ed. (American Psychiatric Publishing, 2013), 10.1176/appi.books.9780890425596. doi.org/10.1176/appi.books.9780890425596
- World Health Organization , Global Status Report on Alcohol and Health 2018 [Internet] (World Health Organization, 2019), 472,https://www.who.int/publications/i/item/9789241565639.
- Office for National Statistics , “Alcohol‐Specific Deaths in the UK: Registered in 2023 [Internet],” 2025,https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/causesofdeath/bulletins/alcoholrelateddeathsintheunitedkingdom/registeredin2023#rate‐of‐alcohol‐specific‐deaths‐in‐the‐uk.
- Saunders H. and Rudowitz R., A Look at the Latest Alcohol Death Data and Change Over the Last Decade [Internet] (KFF, 2024),https://www.kff.org/mental‐health/issue‐brief/a‐look‐at‐the‐latest‐alcohol‐death‐data‐and‐change‐over‐the‐last‐decade/.
- White A. M., Castle I. J. P., Powell P. A., Hingson R. W., and Koob G. F., “Alcohol‐Related Deaths During the COVID‐19 Pandemic,” Journal of the American Medical Association 327, no. 17 (2022): 1704–1706. doi.org/10.1001/jama.2022.4308
- Nuffield Trust , Alcohol‐Related Harm and Drinking Behaviour [Internet] (Nuffield Trust & The Health Foundation, 2023),https://www.nuffieldtrust.org.uk/resource/alcohol‐related‐harm‐and‐drinking‐behaviour‐1.
- Connolly D. J., Copeland C. S., Holland A., Williams A. D., and Shorter G. W., “Exclusion of LGBTQ+ People From the UK'S Alcohol and Other Drug‐Related Death Response,” International Journal of Drug Policy 151 (2026): 105219, 10.1016/j.drugpo.2026.105219. doi.org/10.1016/j.drugpo.2026.105219
- Karaye I. M., Maleki N., Hassan N., and Yunusa I., “Trends in Alcohol‐Related Deaths by Sex in the US, 1999‐2020,” JAMA Network Open 6, no. 7 (2023): e2326346. doi.org/10.1001/jamanetworkopen.2023.26346
- Askgaard G., Leon D. A., Deleuran T., and Tolstrup J. S., “Hospital Admissions and Mortality in the 15 Years After a First‐Time Hospital Contact With an Alcohol Problem: A Prospective Cohort Study Using the Entire Danish Population,” International Journal of Epidemiology 49, no. 1 (February 2020): 94–102. doi.org/10.1093/ije/dyz159
- Green M. A., Strong M., Conway L., and Maheswaran R., “Trends in Alcohol‐Related Admissions to Hospital by Age, Sex and Socioeconomic Deprivation in England, 2002/03 to 2013/14,” BMC Public Health 17, no. 1 (May 2017): 412. doi.org/10.1186/s12889-017-4265-0
- White A. M., “Gender Differences in the Epidemiology of Alcohol Use and Related Harms in the United States,” Alcohol Research: Current Reviews 40, no. 2 (October 2020): 1. doi.org/10.35946/arcr.v40.2.01
- Kirpich I. A., McClain C. J., Vatsalya V., et al., “Liver Injury and Endotoxemia in Male and Female Alcohol‐Dependent Individuals Admitted to an Alcohol Treatment Program,” Alcoholism, Clinical and Experimental Research 41, no. 4 (2017): 747–757. doi.org/10.1111/acer.13346
- Nolen‐Hoeksema S., “Gender Differences in Risk Factors and Consequences for Alcohol Use and Problems,” Clinical Psychology Review 24, no. 8 (December 2004): 981–1010. doi.org/10.1016/j.cpr.2004.08.003
- Cao Y., Willett W. C., Rimm E. B., Stampfer M. J., and Giovannucci E. L., “Light to Moderate Intake of Alcohol, Drinking Patterns, and Risk of Cancer: Results From Two Prospective US Cohort Studies,” BMJ 351 (August 2015): h4238. doi.org/10.1136/bmj.h4238
- Kezer C. A., Simonetto D. A., and Shah V. H., “Sex Differences in Alcohol Consumption and Alcohol‐Associated Liver Disease,” Mayo Clinic Proceedings 96, no. 4 (2021): 1006–1016. doi.org/10.1016/j.mayocp.2020.08.020
- Verplaetse T. L., Carretta R. F., Struble C. A., et al., “Gender Differences in Alcohol Use Disorder Trends From 2009‐2019: An Intersectional Analysis,” Alcohol 123 (March 2025): 101–107. doi.org/10.1016/j.alcohol.2024.11.003
- Kim A. M., Tingen C. M., and Woodruff T. K., “Sex Bias in Trials and Treatment Must End,” Nature 465, no. 7299 (June 2010): 688–689. doi.org/10.1038/465688a
- Shansky R. M., “Are Hormones a ‘Female Problem’ for Animal Research?,” Science 364, no. 6443 (May 2019): 825–826. doi.org/10.1126/science.aaw7570
- Department of Health & Social Care. GOV.UK , “Women's Health Strategy for England,” 2022,https://www.gov.uk/government/publications/womens‐health‐strategy‐for‐england/womens‐health‐strategy‐for‐england.
- Schick M. R., Spillane N. S., and Hostetler K. L., “A Call to Action: A Systematic Review Examining the Failure to Include Females and Members of Minoritized Racial/Ethnic Groups in Clinical Trials of Pharmacological Treatments for Alcohol Use Disorder,” Alcoholism, Clinical and Experimental Research 44, no. 10 (2020): 1933–1951. doi.org/10.1111/acer.14440
- Green R., Roche D. J. O., and Ray L. A., “The Effects of Menstrual Cycle Hormones on Responses to Varenicline and Naltrexone Among Female Heavy Drinking Smokers,” Alcohol and Alcoholism 57, no. 5 (September 2022): 609–614. doi.org/10.1093/alcalc/agac017
- Roche D. J. O. and King A. C., “Sex Differences in Acute Hormonal and Subjective Response to Naltrexone: The Impact of Menstrual Cycle Phase,” Psychoneuroendocrinology 52 (February 2015): 59–71. doi.org/10.1016/j.psyneuen.2014.10.013
- McKee S. A. and McRae‐Clark A. L., “Consideration of Sex and Gender Differences in Addiction Medication Response,” Biology of Sex Differences 13, no. 1 (December 2022): 34. doi.org/10.1186/s13293-022-00441-3
- Zucker R. A., “Alcohol Use and the Alcohol Use Disorders: A Developmental‐Biopsychosocial Systems Formulation Covering the Life Course,” in Developmental Psychopathology [Internet] (John Wiley & Sons, Ltd, 2015), 620–656, 10.1002/9780470939406.ch17. doi.org/10.1002/9780470939406.ch17
- Kirsch D. E., Belnap M. A., Burnette E. M., Grodin E. N., and Ray L. A., “Pharmacological Treatments for Alcohol Use Disorder: Considering the Role of Sex and Gender,” Current Addiction Reports 11, no. 1 (February 2024): 81–93.
- Abulseoud O. A., Karpyak V. M., Schneekloth T., et al., “A Retrospective Study of Gender Differences in Depressive Symptoms and Risk of Relapse in Patients With Alcohol Dependence,” American Journal on Addictions 22, no. 5 (2013): 437–442. doi.org/10.1111/j.1521-0391.2013.12021.x
- Boykoff N., Schneekloth T. D., Hall‐Flavin D., et al., “Gender Differences in the Relationship Between Depressive Symptoms and Cravings in Alcoholism,” American Journal on Addictions 19, no. 4 (2010): 352–356. doi.org/10.1111/j.1521-0391.2010.00057.x
- Logge W., Baillie A., Haber P., Towers E., Riordan B. C., and Morley K., “Sex Differences in the Interrelations Between Stress, Craving and Alcohol Consumption Across Individuals and Time During Baclofen Treatment for Alcohol Dependence,” Addictive Behaviors 136 (January 2023): 107462. doi.org/10.1016/j.addbeh.2022.107462
- Greaves L., “Missing in Action: Sex and Gender in Substance Use Research,” International Journal of Environmental Research and Public Health 17, no. 7 (January 2020): 2352. doi.org/10.3390/ijerph17072352
- Holzhauer C. G., Cucciare M., and Epstein E. E., “Sex and Gender Effects in Recovery From Alcohol Use Disorder,” Alcohol Research: Current Reviews 40, no. 3 (November 2020): 3. doi.org/10.35946/arcr.v40.3.03
- Page M. J., McKenzie J. E., Bossuyt P. M., et al., “The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews,” BMJ 372 (2021): n71, 10.1136/bmj.n71. doi.org/10.1136/bmj.n71
- Bartz D., Chitnis T., Kaiser U. B., et al., “Clinical Advances in Sex‐ and Gender‐Informed Medicine to Improve the Health of All: A Review,” JAMA Internal Medicine 180, no. 4 (April 2020): 574–583. doi.org/10.1001/jamainternmed.2019.7194
- Becher E. and Oertelt‐Prigione S., “The Impact of Sex and Gender in Medicine and Pharmacology,” in Sex and Gender Effects in Pharmacology [Internet], ed. Tsirka S. E. and Acosta‐Martinez M. (Springer International Publishing, 2023), 3–23, 10.1007/164_2023_688. doi.org/10.1007/164_2023_688
- Cheng H. Y., McGuinness L. A., Elbers R. G., et al., “Treatment Interventions to Maintain Abstinence From Alcohol in Primary Care: Systematic Review and Network Meta‐Analysis,” BMJ 371 (November 2020): m3934. doi.org/10.1136/bmj.m3934
- Sterne J. A. C., Savović J., Page M. J., et al., “RoB 2: A Revised Tool for Assessing Risk of Bias in Randomised Trials,” BMJ 366 (August 2019): l4898. doi.org/10.1136/bmj.l4898
- Moola S., Munn Z., Tufanaru C., et al., “Systematic Reviews of Etiology and Risk,” in JBI Manual for Evidence Synthesis [Internet], ed. Aromataris E., Lockwood C., Porritt K., Pilla B., and Jordan Z. (JBI, 2020),https://synthesismanual.jbi.global.
- Schünemann H. J., Higgins J. P., Vist G. E., et al., “Completing ‘Summary of Findings’ Tables and Grading the Certainty of the Evidence,” in Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed. (John Wiley & Sons, 2019), 375–402.
- Popay J., Roberts H., Sowden A., et al., Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product From the ESRC Methods Programme, (Lancaster University, 2006), 10.13140/2.1.1018.4643. doi.org/10.13140/2.1.1018.4643
- Fu R., Gartlehner G., Grant M., et al., “Conducting Quantitative Synthesis When Comparing Medical Interventions: AHRQ and the Effective Health Care Program,” in Methods Guide for Effectiveness and Comparative Effectiveness Reviews [Internet] (Agency for Healthcare Research and Quality (US), 2008), AHRQ Methods for Effective Health Care,http://www.ncbi.nlm.nih.gov/books/NBK49407/.
- Higgins J. P. T., Thompson S. G., Deeks J. J., and Altman D. G., “Measuring Inconsistency in Meta‐Analyses,” BMJ 327, no. 7414 (September 2003): 557–560. doi.org/10.1136/bmj.327.7414.557
- Buri C., Moggi F., Giovanoli A., and Strik W., “Prescription Procedures in Medication for Relapse Prevention After Inpatient Treatment for Alcohol Use Disorders in Switzerland,” Alcohol and Alcoholism 42, no. 4 (May 2007): 333–339. doi.org/10.1093/alcalc/agm038
- Crits‐Christoph P., Markell H. M., Gibbons M. B. C., et al., “A Naturalistic Evaluation of Extended‐Release Naltrexone in Clinical Practice in Missouri,” Journal of Substance Abuse Treatment 70 (2016): 50–57. doi.org/10.1016/j.jsat.2016.07.014
- De Beaurepaire R., “Suppression of Alcohol Dependence Using Baclofen: A 2‐Year Observational Study of 100 Patients,” Frontiers in Psychiatry 3 (2012): 103, 10.3389/fpsyt.2012.00103. doi.org/10.3389/fpsyt.2012.00103
- Flannery B. A., Garbutt J. C., Cody M. W., et al., “Baclofen for Alcohol Dependence: A Preliminary Open‐Label Study,” Alcoholism, Clinical and Experimental Research 28, no. 10 (October 2004): 1517–1523. doi.org/10.1097/01.alc.0000141640.48924.14
- Yoon G., Kim S. W., Petrakis I. L., and Westermeyer J., “High‐Dose Naltrexone Treatment and Gender in Alcohol Dependence,” Clinical Neuropharmacology 39, no. 4 (2016): 165–168. doi.org/10.1097/WNF.0000000000000152
- Korthuis P. T., Lum P. J., Vergara‐Rodriguez P., et al., “Feasibility and Safety of Extended‐Release Naltrexone Treatment of Opioid and Alcohol Use Disorder in HIV Clinics: A Pilot/Feasibility Randomized Trial,” Addiction 112, no. 6 (June 2017): 1036–1044. doi.org/10.1111/add.13753
- Adamson S. J., Sellman J. D., Foulds J. A., et al., “A Randomized Trial of Combined Citalopram and Naltrexone for Nonabstinent Outpatients With co‐Occurring Alcohol Dependence and Major Depression,” Journal of Clinical Psychopharmacology 35, no. 2 (April 2015): 143–149. doi.org/10.1097/JCP.0000000000000287
- Baros A. M., Latham P. K., and Anton R. F., “Naltrexone and Cognitive Behavioral Therapy for the Treatment of Alcohol Dependence: Do Sex Differences Exist?,” Alcoholism, Clinical and Experimental Research 32, no. 5 (May 2008): 771–776. doi.org/10.1111/j.1530-0277.2008.00633.x
- Bold K. W., Zweben A., Fucito L. M., et al., “Longitudinal Findings From a Randomized Clinical Trial of Varenicline for Alcohol Use Disorder With Comorbid Cigarette Smoking,” Alcoholism, Clinical and Experimental Research 43, no. 5 (May 2019): 937–944. doi.org/10.1111/acer.13994
- Davis L., Petrakis I., Pilkinton P., et al., “Comorbid Alcohol Use Disorder and Posttraumatic Stress Disorder: A Proof‐of‐Concept Randomized Placebo‐Controlled Trial of Buprenorphine and Naltrexone Combination Treatment,” Alcoholism, Clinical and Experimental Research 47, no. 9 (2023): 1756–1772. doi.org/10.1111/acer.15155
- Falk D. E., Castle I. J. P., Ryan M., Fertig J., and Litten R. Z., “Moderators of Varenicline Treatment Effects in a Double‐Blind, Placebo‐Controlled Trial for Alcohol Dependence: An Exploratory Analysis,” Journal of Addiction Medicine 9, no. 4 (July 2015): 296–303. doi.org/10.1097/ADM.0000000000000133
- Fertig J. B., Ryan M. L., Falk D. E., et al., “A Double‐Blind, Placebo‐Controlled Trial Assessing the Efficacy of Levetiracetam Extended‐Release in Very Heavy Drinking Alcohol‐Dependent Patients,” Alcoholism, Clinical and Experimental Research 36, no. 8 (August 2012): 1421–1430. doi.org/10.1111/j.1530-0277.2011.01716.x
- Garbutt J. C., “Efficacy and Tolerability of Long‐Acting Injectable Naltrexone for Alcohol Dependence: A Randomized Controlled Trial,” JAMA 106, no. 1 (July 2005): 192. doi.org/10.1001/jama.293.13.1617
- Garbutt J. C., Kampov‐Polevoy A. B., Gallop R., Kalka‐Juhl L., and Flannery B. A., “Efficacy and Safety of Baclofen for Alcohol Dependence: A Randomized, Double‐Blind, Placebo‐Controlled Trial,” Alcoholism: Clinical and Experimental Research 34, no. 11 (November 2010): 1849–1857. doi.org/10.1111/j.1530-0277.2010.01273.x
- Garbutt J. C., Kampov‐Polevoy A. B., Pedersen C., et al., “Efficacy and Tolerability of Baclofen in a U.S. Community Population With Alcohol Use Disorder: A Dose‐Response, Randomized, Controlled Trial,” Neuropsychopharmacology 46, no. 13 (December 2021): 2250–2256. doi.org/10.1038/s41386-021-01055-w
- Goldstein S., Race and Sex Assigned at Birth as Moderators of Harm Reduction Pharmacobehavioural Treatment Outcomes for Alcohol Use Disorder Among People Experiencing Homelessness [Internet], ed. Kingston R. I. (University of Rhode Island, 2023),https://digitalcommons.uri.edu/oa_diss/1580.
- Hashimoto N., Habu H., Takao S., et al., “Clinical Moderators of Response to Nalmefene in a Randomized‐Controlled Trial for Alcohol Dependence: An Exploratory Analysis,” Drug and Alcohol Dependence 233 (April 2022): 109365. doi.org/10.1016/j.drugalcdep.2022.109365
- Krystal J. H. and Rosenheck R. A., “Naltrexone in the Treatment of Alcohol Dependence,” New England Journal of Medicine 345 (2001): 1734–1739. doi.org/10.1056/NEJMoa011127
- Mason B. J. and Lehert P., “Acamprosate for Alcohol Dependence: A Sex‐Specific Meta‐Analysis Based on Individual Patient Data,” Alcoholism, Clinical and Experimental Research 36, no. 3 (2012): 497–508. doi.org/10.1111/j.1530-0277.2011.01616.x
- Morley K. C., Louie E., Hurzeler T., et al., “Sex as a Potential Moderator for Baclofen Response in the Treatment of Alcohol Dependence,” Frontiers in Global Women's Health 3 (March 2022): 807269. doi.org/10.3389/fgwh.2022.807269
- Naranjo C. A., Knoke D. M., and Bremner K. E., “Variations in Response to Citalopram in Men and Women With Alcohol Dependence,” Journal of Psychiatry & Neuroscience 25 (2000): 269–275.
- O'Malley S. S., Zweben A., Fucito L. M., et al., “Effect of Varenicline Combined With Medical Management on Alcohol Use Disorder With Comorbid Cigarette Smoking: A Randomized Clinical Trial,” JAMA Psychiatry 75, no. 2 (February 2018): 129–138. doi.org/10.1001/jamapsychiatry.2017.3544
- Pettinati H. M., Kampman K. M., Lynch K. G., et al., “Gender Differences With High‐Dose Naltrexone in Patients With Co‐Occurring Cocaine and Alcohol Dependence,” Journal of Substance Abuse Treatment 34, no. 4 (June 2008): 378–390. doi.org/10.1016/j.jsat.2007.05.011
- Reynaud M., Aubin H. J., Trinquet F., et al., “A Randomized, Placebo‐Controlled Study of High‐Dose Baclofen in Alcohol‐Dependent Patients—The ALPADIR Study,” Alcohol and Alcoholism 52, no. 4 (July 2017): 439–446. doi.org/10.1093/alcalc/agx030
- Stoner S. A., Arenella P. B., and Hendershot C. S., “Randomized Controlled Trial of a Mobile Phone Intervention for Improving Adherence to Naltrexone for Alcohol Use Disorders,” PLoS One 10, no. 4 (April 2015): e0124613. doi.org/10.1371/journal.pone.0124613
- Wiesbeck G. A., Weijers H. G., Wodarz N., Lesch O. M., Glaser T., and Boening J., “Gender‐Related Differences in Pharmacological Relapse Prevention With Flupenthixol Decanoate in Detoxified Alcoholics,” Archives of Women's Mental Health 6, no. 4 (November 2003): 259–262. doi.org/10.1007/s00737-003-0010-z
- Witte J., Bentley K., Evins A. E., et al., “A Randomized, Controlled, Pilot Study of Acamprosate Added to Escitalopram in Adults With Major Depressive Disorder and Alcohol Use Disorder,” Journal of Clinical Psychopharmacology 32, no. 6 (December 2012): 787–796. doi.org/10.1097/JCP.0b013e3182726764
- Greenfield S. F., Pettinati H. M., O'Malley S., Randall P. K., and Randall C. L., “Gender Differences in Alcohol Treatment: An Analysis of Outcome From the COMBINE Study,” Alcoholism, Clinical and Experimental Research 34, no. 10 (October 2010): 1803–1812. doi.org/10.1111/j.1530-0277.2010.01267.x
- Naranjo C. A., Knoke D. M., and Bremner K. E., “Variations in Response to Citalopram in Men and Women With Alcohol Dependence,” Journal of Psychiatry and Neuroscience 25, no. 3 (May 2000): 269–275.
- Jarvis B. P., Holtyn A. F., Subramaniam S., et al., “Extended‐Release Injectable Naltrexone for Opioid Use Disorder: A Systematic Review,” Addiction 113, no. 7 (2018): 1188–1209. doi.org/10.1111/add.14180
- Benjamin D., Grant E. R., and Pohorecky L. A., “Naltrexone Reverses Ethanol‐Induced Dopamine Release in the Nucleus Accumbens in Awake, Freely Moving Rats,” Brain Research 621, no. 1 (1993): 137–140. doi.org/10.1016/0006-8993(93)90309-b
- Thorsell A., “The μ‐Opioid Receptor and Treatment Response to Naltrexone,” Alcohol and Alcoholism 48, no. 4 (July 2013): 402–408. doi.org/10.1093/alcalc/agt030
- Mann K., Roos C. R., Hoffmann S., et al., “Precision Medicine in Alcohol Dependence: A Controlled Trial Testing Pharmacotherapy Response Among Reward and Relief Drinking Phenotypes,” Neuropsychopharmacology 43, no. 4 (March 2018): 891–899. doi.org/10.1038/npp.2017.282
- Becker J. B., Perry A. N., and Westenbroek C., “Sex Differences in the Neural Mechanisms Mediating Addiction: A New Synthesis and Hypothesis,” Biology of Sex Differences 3, no. 1 (June 2012): 14. doi.org/10.1186/2042-6410-3-14
- Lehavot K., Stappenbeck C. A., Luterek J. A., Kaysen D., and Simpson T. L., “Gender Differences in Relationships Among PTSD Severity, Drinking Motives, and Alcohol Use in a Comorbid Alcohol Dependence and PTSD Sample,” Psychology of Addictive Behaviors 28, no. 1 (2014): 42–52. doi.org/10.1037/a0032266
- Rochat L., Rothen S., Edel Y., et al., “Measurement Invariance of the Marijuana Motives Measure Among Men and Women Using Stop Cannabis App,” Addictive Behaviors 148 (January 2024): 107866. doi.org/10.1016/j.addbeh.2023.107866
- Liu J. C., Ma J. D., Morello C. M., Atayee R. S., and Best B. M., “Naltrexone Metabolism and Concomitant Drug Concentrations in Chronic Pain Patients,” Journal of Analytical Toxicology 38, no. 4 (May 2014): 212–217. doi.org/10.1093/jat/bku019
- Guinle M. I. B. and Sinha R., “The Role of Stress, Trauma, and Negative Affect in Alcohol Misuse and Alcohol Use Disorder in Women,” Alcohol Research: Current Reviews 40, no. 2 (August 2020): 5. doi.org/10.35946/arcr.v40.2.05
- Peltier M. R., Verplaetse T. L., Mineur Y. S., et al., “Sex Differences in Stress‐Related Alcohol Use,” Neurobiology of Stress 10 (February 2019): 100149. doi.org/10.1016/j.ynstr.2019.100149
- Kuntsche E., Wicki M., Windlin B., et al., “Drinking Motives Mediate Cultural Differences but Not Gender Differences in Adolescent Alcohol Use,” Journal of Adolescent Health 56, no. 3 (March 2015): 323–329. doi.org/10.1016/j.jadohealth.2014.10.267
- Kuntsche E. and Labhart F., “Drinking Motives Moderate the Impact of Pre‐Drinking on Heavy Drinking on a Given Evening and Related Adverse Consequences—An Event‐Level Study,” Addiction 108, no. 10 (2013): 1747–1755. doi.org/10.1111/add.12253
- Agabio R. and Leggio L., “Baclofen in the Treatment of Patients With Alcohol Use Disorder and Other Mental Health Disorders,” Frontiers in Psychiatry 9 (September 2018): 464, 10.3389/fpsyt.2018.00464/full. doi.org/10.3389/fpsyt.2018.00464/full
- Tyacke R. J., Lingford‐Hughes A., Reed L. J., and Nutt D. J., “GABAB Receptors in Addiction and Its Treatment,” in Advances in Pharmacology [Internet]. GABAReceptor Pharmacology, vol. 58, ed. Blackburn T. P. (Academic Press, 2010), 373–396,https://www.sciencedirect.com/science/article/pii/S1054358910580141. doi.org/10.1016/S1054-3589(10)58014-1
- Agabio R., Baldwin D. S., Amaro H., Leggio L., and Sinclair J. M. A., “The Influence of Anxiety Symptoms on Clinical Outcomes During Baclofen Treatment of Alcohol Use Disorder: A Systematic Review and Meta‐Analysis,” Neuroscience and Biobehavioral Reviews 125 (June 2021): 296–313. doi.org/10.1016/j.neubiorev.2020.12.030
- Heidari S., Babor T. F., De Castro P., Tort S., and Curno M., “Sex and Gender Equity in Research: Rationale for the SAGER Guidelines and Recommended Use,” Research Integrity and Peer Review 1, no. 1 (May 2016): 2. doi.org/10.1186/s41073-016-0007-6
- Van Epps H., Astudillo O., Del Pozo M. Y., and Marsh J., “The Sex and Gender Equity in Research (SAGER) Guidelines: Implementation and Checklist Development,” European Science Editing 5, no. 48 (October 2022): e86910. doi.org/10.12771/emj.2024.e11
- Williams A. D. N., Hood K., Bracken K., and Shorter G. W., “The Importance of NOT Being Other: Time to Address the Invisibility of Nuanced Gender and Sexuality in Clinical Trials,” Trials 24, no. 1 (March 2023): 242. doi.org/10.1186/s13063-023-07278-0
- Humphreys K., Weingardt K. R., and Harris A. H. S., “Influence of Subject Eligibility Criteria on Compliance With National Institutes of Health Guidelines for Inclusion of Women, Minorities, and Children in Treatment Research,” Alcoholism, Clinical and Experimental Research 31, no. 6 (2007): 988–995. doi.org/10.1111/j.1530-0277.2007.00391.x
- Waltz M., Lyerly A. D., and Fisher J. A., “Exclusion of Women From Phase I Trials: Perspectives From Investigators and Research Oversight Officials,” Ethics & Human Research 45, no. 6 (2023): 19–30. doi.org/10.1002/eahr.500170
- Dahlberg M., Boson K., Anderberg M., and Wennberg P., “Long‐Term Outcomes for Young People With Substance Use Problems in Outpatient Treatment: Gender‐Specific Patterns,” Frontiers in Psychiatry 13 (2022): 888197, 10.3389/fpsyt.2022.888197/full. doi.org/10.3389/fpsyt.2022.888197/full
- Shorter G. W., Bray J. W., Giles E. L., et al., “The Variability of Outcomes Used in Efficacy and Effectiveness Trials of Alcohol Brief Interventions: A Systematic Review,” Journal of Studies on Alcohol and Drugs 80, no. 3 (May 2019): 286–298.
- Shorter G. W., Bray J. W., Heather N., et al., “The ‘Outcome Reporting in Brief Intervention Trials: Alcohol’ (ORBITAL) Core Outcome Set: International Consensus on Outcomes to Measure in Efficacy and Effectiveness Trials of Alcohol Brief Interventions,” Journal of Studies on Alcohol and Drugs 82, no. 5 (September 2021): 638–646. doi.org/10.15288/jsad.2021.82.638
Republished from the open web under CC-BY. Authors: Allen J, Jones A, Shorter GW, Montgomery C, Kougiali Z, Bagnall A, Adshead C, Smith J, Burton S, Atkinson A, Guelen L, Rose A. Read the original.