Sense of School Belonging and School Reintegration for Students Hospitalized With Chronic or Complex Medical Diseases: Insights From a Grounded Theory Study.
Background A strong sense of school belonging (SoSB) supports students' emotional well-being, engagement, and adjustment. For students hospitalized because of chronic or complex conditions, maintaining SoSB is challenging yet essential for successful school reintegration. Methods Using a Grounded Theory approach, this study combined interviews with 16 parents, 32 mainstream teachers, 31 hospital teachers, and one association, alongside drawings from 14 hospitalized students. Data were collected pre- and post-COVID-19. Drawings were analyzed through a meaning-making approach, and all materials underwent iterative coding and constant comparison. Results Students reported strong emotional bonds with hospital teachers but felt forgotten by their mainstream schools. Peer contact was limited, and teachers felt unprepared to manage absences and reintegration. Structural gaps and weak communication between schools hindered continuity. Both formal (e.g., remote lessons) and informal (e.g., messages, drawings) exchanges, along with psychologists and associations, emerged as protective factors. Implications for school health policy, practice, and equity Findings highlight the need for integrated school-health policies, teacher training, and structured collaboration to ensure equitable relational continuity. Conclusions Promoting SoSB during hospitalization is crucial for recovery, resilience, and educational equity.
Background
Children and adolescents with chronic or complex diseases often experience prolonged hospitalization, disrupting daily routines and living apart from their homes, schools, and social environments. A biopsychosocial and ecological perspective highlights how illness affects development across physical, psychological, and social domains [1,2]. Illness as a biographical disruption generates interconnected challenges, including medical burdens such as fatigue and treatment side effects, psychological vulnerabilities such as anxiety and reduced self‐efficacy, and social disruptions linked to separation from peers and school life [3,4,5,6,7,8].
These conditions may lead to fear, isolation, and trauma [9,10,11,12,13], as well as impair academic performance and self‐esteem [7,14,15]. Children with medical conditions are also at higher risk of bullying, often exacerbated by stigma and limited peer awareness of the child's medical condition [16,17]. Protective factors such as supportive peer relationships, effective school–home–hospital communication, and inclusive practices can buffer these risks. Teachers may likewise experience stress and burnout, particularly in the absence of adequate training on this matter and institutional support [18,19,20].
Maintaining school connection during hospitalization is crucial for students' well‐being and reintegration [21]. Hospital‐based schools aim to ensure educational continuity through individualized instruction adapted to students' medical conditions. Hospital teachers play a key role within these settings, providing individualized instruction, liaising with mainstream schools, and supporting students' emotional adjustment during hospitalization and school reintegration [22]. Within this context, the sense of school belonging (SoSB) represents a key construct. Defined as feeling valued and connected to the school environment, SoSB is associated with emotional well‐being, academic success, and social development [23,24,25].
Higher SoSB is linked to reduced distress and stronger relationships [26,27,28], whereas prolonged absence and limited communication may undermine sense of belonging [20,29,30,31,32].
Recent literature conceptualizes SoSB as a multifaceted construct encompassing relational, organizational, and technological dimensions [30,33,34], including peer and teacher relationships [35], participation in school life, continuity practices between hospital‐ and mainstream schools, and the use of digital technologies [20,30]. Growing evidence identifies SoSB as a facilitator of well‐being and academic and psychological outcomes among students with chronic illness [32,36,37,38,39]. Alongside this focus, European child‐rights frameworks emphasize the inclusion of children's voices in research and practice, promoting narrative and meaning‐making methods to capture children's experiences within their broader social ecology [40,41].
Despite extensive research on academic and emotional outcomes of pediatric illness [42], limited attention has been devoted to how hospitalized students maintain connections with their school communities, and few studies integrate children's voices alongside those of parents and teachers [43]. Addressing this gap is essential to understanding how school belonging is sustained during hospitalization and reintegration.
Aims of the Research
The aim of this research is to explore the connection between hospitalized students and their classmates, with a particular focus on understanding the role thatSense of School Belonging(SoSB) plays in the school experience of students with chronic medical diseases. To date, no studies have examined this aspect.
Methods
The study received ethical approval from institutional ethics committees overseeing the different phases of data collection. All procedures were conducted in accordance with approved protocols and ethical guidelines for research involving minors and vulnerable populations. Written informed consent was obtained from all adult participants and from parents or legal guardians of participating children, and assent was obtained from children in an age‐appropriate manner. Data were collected and stored in anonymized and aggregated form to ensure participants' confidentiality and privacy. Particular care was taken in handling sensitive materials, including children's drawings and narratives, to prevent identification.
This study adopted a grounded theory methodology, a qualitative approach suited to under‐explored phenomena and inductive conceptual development. Grounded theory guided sampling, data collection, and iterative coding procedures [44,45,46]. Semi‐structured and long interviews with parents and teachers were analyzed through grounded theory coding phases to identify recurrent patterns and higher‐order categories. To complement this process, children's drawings were examined using a meaning‐making approach, enabling access to children's subjective experiences in a developmentally appropriate way [40,41,42,43,44,45,46,47,48,49,50]. Five participant groups were involved: hospitalized students, parents, mainstream teachers, hospital teachers, and an association that promotes school inclusion. The association was included as its relevance emerged during early analysis and the evolving COVID‐19 context. Students and parents were interviewed only pre‐COVID, while mainstream and hospital teachers were interviewed both pre‐COVID (Time 1) and post‐lockdown (Time 2).
Participants
Fourteen hospitalized students (8 males, 6 females; ages 8–12, M = 9.93) were recruited from oncology (79%) and general pediatric (21%) wards. Sixteen parents (87.5% females) participated. Thirty‐two mainstream teachers and thirty‐one hospital schoolteachers took part across the two phases. One regional association focused on educational inclusion was involved post‐pandemic.
Research Tools and Procedure
Children produced two open‐ended drawings representing hospital‐based and mainstream school experiences. Drawings are widely used to explore children's emotions and meaning‐making around illness and schooling [51,52,53]. No content instructions or time limits were provided, and materials were freely chosen. Methodological rigor was maintained throughout data collection and analysis. Each drawing was independently examined by two researchers and discussed through interpretative triangulation to enhance analytical credibility [46,54].
Parents participated in semi‐structured interviews, adapted to the hospital context, exploring school–hospital connections, school roles, educational continuity, and transition challenges.
Mainstream and hospital teachers and the association took part in long‐form interviews. Pre‐COVID teachers were randomly selected, while post‐COVID participants were voluntary. Hospital teachers were identified through regional mapping of hospital education services. The association was identified through a systematic mapping of regional organizations, with the identification independently verified by the research team.
The overall methodological framework of the study, including participant groups, recruitment procedures, instruments, timing of data collection, and analytic approach, is summarized in Figure1.
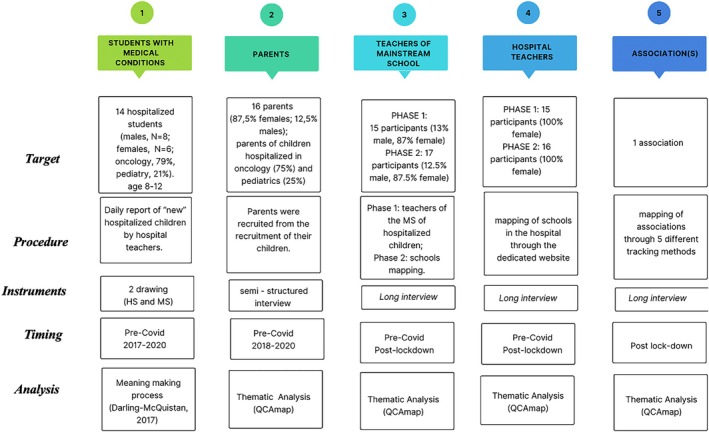
Summary of the research methodology.
Data Analysis
Researchers first conducted a descriptive analysis of the drawings to identify similarities and differences. This analysis was further developed using a meaning‐making approach, in which children were invited to explain their drawings and their narratives were recorded [48,55]. Researchers used open‐ended questions to encourage children's free expression and elaboration [56]. Consistent with this approach, the analysis privileged children's subjective interpretations rather than external adult readings [49].
For the semi‐structured and long interviews, data were analyzed using grounded theory coding procedures (open, axial, and selective coding) [46], supported by QCAMAP software. Consistent with grounded theory principles, categories emerged through an inductive constant comparative process [57,58]. Both drawing and interview analyses were embedded within the same grounded theory framework. To enhance trustworthiness, at least two researchers independently coded the material and discussed interpretations through researcher triangulation [54].
Results
Illustrative participant quotes supporting each emerging category are reported in Table1.
Table: Illustrative quotes linked to emerging categories.
Emotions in Participation During Hospital School Activities
The data highlighted how the hospital school (HBS) can foster future orientation, provide a sense of normalcy, act as a distraction from illness, and maintain connections with the student's mainstream school (MS). Overall, HBS was described by parents and teachers as promoting continuity in education and facilitating smoother school reintegration. Hospital teachers emphasized that HBS helps students feel less isolated and more “equal to their peers,” while supporting healthy aspects of identity development through everyday activities, personal growth, and life skills beyond academic learning. HBS was also reported to promote children's autonomy and emotional separation from parents during hospitalization, helping preserve their identity as students. Parents considered this particularly important given the regression in independence often associated with illness, whereas teachers highlighted the central role of collaboration between hospital, school, and family in sustaining school belonging.
Finally, participation in HBS contributed to a broader reframing of the meaning of school among both parents and teachers. School was increasingly viewed not only as a place for academic achievement but also as a relational and developmental space, with parents experiencing emotional relief and teachers recognizing the importance of relationships alongside learning.
Relationship Between Hospital School and Mainstream School
Mainstream teachers described communication with the HBS as largely mediated by hospital school coordinators or support services, which often generated feelings of distance and lack of communication and institutional support, particularly at the secondary school level where teacher–student contact is more limited. This delegation contributed to teachers' experiences of isolation and reduced involvement in supporting hospitalized students.
In contrast, hospital teachers perceived limited engagement from mainstream teachers in maintaining school–hospital connections, with some reporting that hospitalized students were sometimes forgotten by mainstream schools, especially when staff changes occurred. Both groups identified a shared challenge in the absence of adequate training to manage school–hospital coordination and foster school belonging.
These relational dynamics highlighted the importance of supportive school relationships in sustaining connection and reintegration. Several teachers described uncertainty and fear of intrusiveness, which often resulted in inaction when a student was hospitalized. In this context, school psychologists emerged as key figures in guiding teachers and facilitating reintegration processes, reinforcing the idea that students remain active members of their school communities throughout hospitalization.
Teacher‐Student Attachment
The findings showed that the relationship between students and hospital schoolteachers differs substantially from that in mainstream schools, primarily due to the one‐to‐one interaction characteristic of the hospital setting. While mainstream teachers typically engage with entire classes and have fewer opportunities for dyadic relationships, the hospital context appears to facilitate the development of a strong emotional bond with hospital teachers across all participant groups.
Children consistently depicted their hospital schoolteachers in their drawings and described close, positive relational experiences, which were also confirmed by parents and hospital teachers. Notably, drawings of the hospital school context focused exclusively on the dyadic teacher–student relationship, with no peers represented. This pattern is illustrated in Figure2, where the hospital school is portrayed as a one‐to‐one interaction beside the hospital bed. In contrast, drawings of mainstream schools often emphasized the physical classroom environment, such as desks and blackboards, and sometimes omitted both teachers and classmates, suggesting a more impersonal representation of the school context.

Children's representations of hospital‐based and mainstream school contexts: dyadic teacher–student interaction versus collective classroom environment.
Sense of School Belonging and School Reintegration: Organizational and Relational Issues
Overall, the findings highlighted significant organizational differences between hospital schools and mainstream schools that may hinder reintegration processes. Hospital teachers emphasized that the specific temporal and spatial constraints of the hospital context require tailored teaching approaches, while mainstream teachers perceived differences between hospital and mainstream teaching methods as creating a disconnect in students' educational experiences and complicating their return to school.
Beyond organizational aspects, the relational dimension emerged as central for students' emotional experiences during hospitalization. Children's drawings and interviews consistently portrayed the HBS as a highly relational context, primarily focused on the dyadic teacher–student relationship rather than on peer interactions. This perception aligned with reports from parents and teachers, who highlighted the role of HBS in fostering feelings of normalcy, equality, and emotional support.
At the same time, the hospital context posed major challenges for implementing collective learning experiences. Limits of group activities in hospital school were reported by hospital teachers, who explained that differences in students' ages, curricula, and length of hospitalization made sustained group teaching difficult, in contrast to mainstream schools where classes share long‐term peer relationships and collective experiences.
In children's drawings, mainstream schools were strongly associated with peer relationships, including both formal classroom moments and informal social interactions. Some children avoided drawing their mainstream school, describing sadness for missing classmates. This experience was echoed by parents and teachers, who reported that hospitalized students often felt forgotten by their schoolmates. Overall, maintaining educational continuity appeared insufficient to sustain a strong sense of school belonging. Figure3provides a visual synthesis of the main dimensions of school belonging that emerged from the analysis, highlighting how relational continuity, teacher–student attachment, participation in class activities, psychological support, and digital tools interact in shaping hospitalized students' school experience.
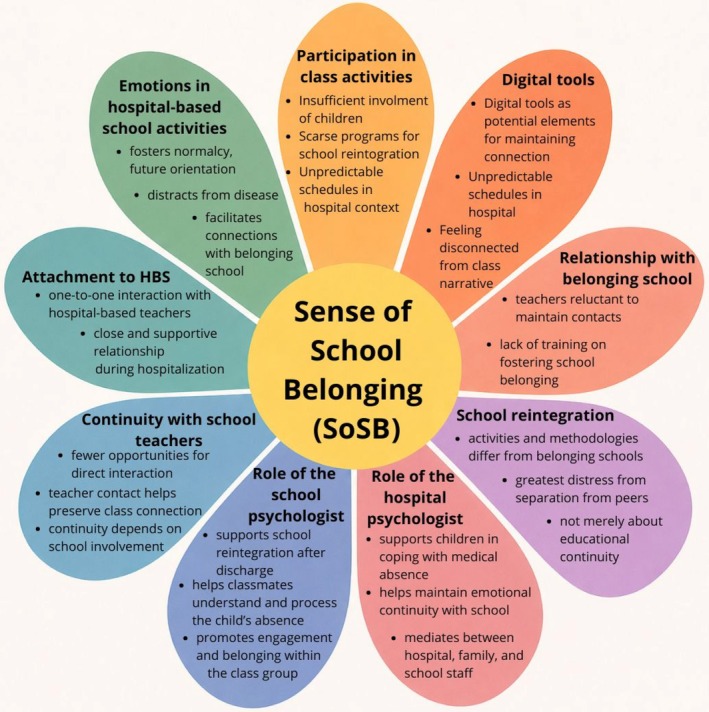
Dimensions of school belonging during hospitalization.
Need for Specific Training for School Staff
The findings revealed substantial gaps in the training of mainstream teachers, who often reported feeling unprepared to manage the complexities of students' illnesses, promote inclusion, and prevent school dropout during medical absence. These difficulties were confirmed by hospital teachers, parents, and students, with children's drawings and narratives reflecting emotional distress and feelings of disconnection from their schools. Parents particularly described challenges in maintaining communication with teachers, especially at the middle school level, while some students avoided drawing their mainstream school due to sadness linked to feeling forgotten.
Despite these challenges, not all mainstream teachers perceived additional training as necessary, arguing that existing competencies in special pedagogy were sufficient. However, these same teachers described difficulties when facing unexpected situations, including parental resistance to maintaining connection, school phobia during reintegration, communication with classmates about illness, managing peers' fears, and coordinating with hospital services.
In contrast, hospital teachers strongly emphasized the importance of specialized training, although many reported they learn primarily through experience rather than formal preparation. While professional development opportunities have increased over time, training remains non‐mandatory and most effective when delivered by professionals with in‐depth knowledge of the HBS context.
Finally, the involved association highlighted the central role of teacher training and network‐building among school, family, and hospital in fostering school belonging. Although the association partially addressed training gaps, the study identified only one local association specifically dedicated to preparing teachers and raising awareness about school inclusion for students with medical conditions.
The Role of the Psychologist in Promoting School Inclusion and Sense of Belonging
Both hospital and mainstream teachers emphasized the central role of psychological support in reintegration, particularly during students' return to school, which was described as one of the most challenging phases of the illness trajectory. Prolonged absences often led hospitalized students to feel disconnected from their classroom communities, undermining their sense of school belonging.
Teachers also reported difficulties in maintaining structured relationships between hospitalized students and their classmates, especially in secondary school, where this responsibility was often left to informal peer interactions. The absence of organized programs supporting reintegration in both formal and informal school contexts further intensified these challenges.
At the same time, teachers expressed concerns about the feasibility of involving psychologists in managing communication about a classmate's illness. Information was frequently shared spontaneously through informal channels such as informal conversations or messaging apps, making it difficult to control or structure. However, teachers acknowledged that while initial communication may be hard to formalize, the subsequent phase of helping students process and understand the situation could be addressed more systematically.
In contrast, the involved association emphasized that structured support across the entire disease trajectory is achievable, provided that effective collaboration and networking between school, family, and hospital are established. From this perspective, current difficulties were linked to the fragmentation of psychological services, which limited continuity of support.
Sense of School Belonging and Participation in Class Activities
The findings highlighted that a strong sense of school belonging requires students' active participation in school life, involvement in the class narrative, and engagement with the symbolic elements of the school environment. When these components are lacking, hospitalized students risk feeling abandoned, misunderstood, and emotionally disconnected from their schools.
Hospitalized students were often insufficiently involved in class activities during prolonged absences, threatening their sense of belonging. Although mainstream teachers frequently reported “being in contact” with hospitalized students, closer examination revealed that communication was primarily maintained with parents or hospital teachers rather than directly with students. This pattern was confirmed by parents and hospital schoolteachers, who described persistent difficulties in sustaining regular and informal school–hospital connections.
When peer contact occurred, it was often spontaneous and student‐started. While some teachers viewed this positively as promoting autonomy and peer relationships, others emphasized that reliance on informal communication frequently resulted in prolonged disengagement and weakened sense of school belonging. Direct contact with hospitalized students was generally infrequent and mainly focused on academic matters rather than relational support.
Hospital teachers further noted that mainstream schools often struggled to address students' relational needs alongside educational plans. Although positive reintegration experiences were reported in some cases, the findings suggested that many students, despite feeling welcomed upon return, did not fully regain their place within the ongoing class narrative they had been part of prior to hospitalization.
Digital Tools to Promote a Sense of School Belonging: Balancing Opportunities and Challenges
All participants emphasized that technology has long been considered essential for maintaining the school–hospital connection, both educationally and relationally. Before the COVID‐19 pandemic, however, mainstream schools and the association had not implemented online educational activities and often perceived such connections as impractical, whereas hospital teachers already believed continuous distance learning was feasible.
In the pre‐pandemic phase, difficulties were mainly attributed to poor internet connectivity and limited digital skills. Although these technical barriers were partially resolved during the pandemic, new and more complex challenges emerged. Teachers reported difficulties integrating hospitalized students into distance and hybrid learning due to medical routines, limited attention in online settings, and challenges in sustaining active participation.
The pandemic experience also revealed the emotional and professional burden on teachers, reducing time and resources for maintaining school–hospital connections. Importantly, it highlighted the irreplaceable role of face‐to‐face presence and meaningful human relationships in supporting hospitalized students. While remote lessons were once considered sufficient to maintain connection, post‐pandemic teachers no longer viewed technology alone as adequate for fostering engagement and a sense of school belonging.
Overall, although COVID‐19 accelerated the adoption of digital tools in education, it did not substantially improve inclusion for hospitalized students, who continued to experience isolation as well as peers affected by lockdowns.
Individual and Relational Emotional Experiences Related to the Pandemic
Teachers reported that some students initially experienced a sense of normalcy during the pandemic, feeling part of a shared experience of isolation. Over time, however, students became increasingly aware of the difference between hospitalization due to illness and lockdown‐related isolation, which heightened feelings of difference and exclusion.
Distance learning reinforced misconceptions among mainstream teachers, who sometimes assumed that HBS was no longer necessary, reflecting the perceived limits of distance learning for maintaining meaningful school–hospital connections. In practice, hospitalized students were included under the same conditions as peers in quarantine, without consideration of their distinct routines and needs, resulting in minimal participation and increased disconnection.
Hospital teachers also described a weakening of student–teacher relationships during remote lessons, particularly in demanding wards, contributing to lower mood and emotional distress among hospitalized children. These experiences reflected the broader impact of COVID‐19 on inclusion practices within hospital education. One positive change involved classmates' parents, whose resistance to school–hospital contact decreased after the pandemic, with greater openness to communication and recorded lessons to support inclusion.
Discussion
The present study underscores the central role of hospital schools in fostering normalcy, future orientation, and educational continuity for hospitalized students. Consistent with research showing that hospital schooling mitigates educational disruption by reinforcing children's identity as learners rather than patients [59,60], our findings demonstrate that HBS functions as a symbolic bridge toward life beyond hospitalization. This aligns with family‐centered interventions emphasizing educational identity [61] and qualitative studies highlighting school as a domain for envisioning a future beyond illness [32].
HBS also promoted personal growth and emotional autonomy through close dyadic teacher–student relationships. In line with attachment‐oriented perspectives, these bonds fostered resilience in medicalized environments [62,63].
Despite recognition of school belonging, fragmentation between hospital and mainstream schools emerged. Limited awareness of HBS, institutional isolation, and insufficient training weakened collaboration. These findings confirm European evidence of systemic disconnection [64] and Italian research showing that pandemic‐driven digital innovation did not resolve relational gaps [64,65]. Fragmentation appeared both structural and relational, reflecting limited institutional recognition of hospital schooling.
A key contribution concerns the redefinition of school belonging in hospital contexts. While belonging in mainstream schooling is largely grounded in peer relationships [66,67], hospitalized students primarily experienced belonging through adult–child dyads with hospital teachers, consistent with individualized pedagogy [68]. Nevertheless, peer connections with the original class community remained crucial, sustaining social identity [69], supporting academic motivation [70], and facilitating school reintegration [33,71]. When continuity was lacking, students experienced isolation and anxiety about returning to school [32].
These findings invite a shift in perspective, positioning the mainstream school as the student'sschool of belonging, rather than simply the place to which they return. From this perspective, students remain part of their school community throughout hospitalization, supporting meaningful inclusion and a smoother reintegration process, in line with recent work on school reentry pathways [30].
Organizational differences between HBS and mainstream schools further complicated reintegration. While HBS emphasizes individualized approaches [68], MS operate within collective classroom structures and standardized curricula, creating barriers to coordination. Although digital technologies were viewed as potential bridges, their effectiveness proved limited when used alone. Post‐pandemic challenges included medical routines, reduced online engagement, and professional fatigue. These findings support concerns regarding digital‐only solutions [38]. While innovative tools have been explored [72,73,74], they remain exploratory. A recent Delphi study suggests that flexible asynchronous tools may offer more balanced approaches [30].
Psychological support emerged as essential during reintegration, aligning with interdisciplinary and systemic models [30,75,76].
Overall, school belonging emerged as a multidimensional construct encompassing academic, relational, and identity‐related processes [33], requiring deliberate support beyond academic continuity.
Limits of the Study
This study has several limitations that should be considered when interpreting the findings. First, the qualitative sample was relatively small and did not include post‐pandemic student participants, limiting the possibility of capturing changes in children's experiences over time. In addition, findings may be context‐specific and not fully transferable to other educational or healthcare systems, particularly given the organizational features of hospital schooling in the European context. The study also relies more extensively on the perspectives of adult informants (parents and teachers), which may have shaped the interpretation of children's experiences despite the inclusion of drawings and narrative accounts.
Nevertheless, the integration of multiple perspectives, the use of complementary qualitative methods, and the application of grounded theory procedures support the robustness of the findings. Moreover, the alignment with belonging theory and child‐rights frameworks [40,41] provides a coherent interpretative lens that recognizes hospitalized children as active participants in their educational and developmental trajectories.
Implications for School Health Policy, Practice, and Equity
This study highlights implications for school health professionals supporting students with complex medical conditions. Maintaining hospitalized students' inclusion within the class experiences and school community is essential to prevent psychological distress during school reintegration. Many students felt forgotten when there was no informal connection with schoolmates and mainstream teachers, even when educational continuity was ensured.
To foster SoSB, collaboration between hospital and mainstream schools should promote both formal connections (e.g., remote lessons) and informal interactions (e.g., messages, peer initiatives). Active participation is necessary, and mainstream teachers should be supported in maintaining meaningful contact.
Targeted training for teachers and staff is crucial, as many felt unprepared to address students' medical and emotional needs. Training should integrate didactic and relational competencies and should be developed with hospital teachers and healthcare professionals.
Psychologists play a central role in communication, emotional support, and reintegration planning and should be systematically involved. External associations can further assist through tailored interventions and awareness initiatives about illness and school reintegration.
While digital tools can facilitate school–hospital connections, they cannot replace relational engagement and must be embedded within meaningful human relationships.
Overall, promoting school belonging requires investment in teacher training, inclusive practices, psychological support, sustained school–hospital collaboration, and clear policy guidelines.
Conclusions
Hospitalization disrupts students' connection with their school communities, placing their sense of school belonging at risk. This study highlights the need to reconceptualize belonging in hospital contexts as relational, organizational, and identity‐based. Supporting school belonging requires coordinated efforts across hospital and mainstream schools, integrating educational, relational, and psychological dimensions to ensure continuity, inclusion, and equity in students' educational trajectories.
Funding
This work was supported by University of Florence (Italy) with a research grant.
Ethics Statement
This study is part of a broader project approved by two ethical committees:pre‐Covid 19 data collection (involving children and parents) was approved by Meyer Pediatric Ethical Committee (n. of register: 08/2019, emendamento n. 4 of 03/01/2019, Prot. Scuola in Ospedale)the second data collection after pandemic was approved by FORLILPSI Department of University of Florence Ethical Commettee (n. SIO_Unifi, parere 138 del 05/02/2021).
As per the protocol submitted to the ethics committee, each research participant signed an informed consent form to take part in the present study. The informed consent form was prepared and approved by the aforementioned ethics committees. The research data are stored in an anonymized and aggregated manner, in accordance with the informed consent and the research protocol forms approved by the ethics committee, to ensure participants' privacy. Further information is available in the records of the ethics committees (in Italian).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- U. Bronfenbrenner, The Ecology of Human Development: Experiments by Nature and Design(Harvard University Press, 1979).
- G. L. Engel, “The Need for a New Medical Model: A Challenge for Biomedicine, ”Science196, no. 4286(1977): 129–136, . doi.org/10.1126/science.847460
- M. Bury, “Chronic Illness as Biographical Disruption, ”Sociology of Health & Illness4, no. 2(1982): 167–182, . doi.org/10.1111/1467-9566.ep11339939
- B. E. Compas, S. S. Jaser, M. J. Dunn, andE. M. Rodriguez, “Coping With Chronic Illness in Childhood and Adolescence, ”Annual Review of Clinical Psychology8, no. 1(2012): 455–480, . doi.org/10.1146/annurev-clinpsy-032511-143108
- C. Crump, D. Rivera, R. London, M. Landau, B. Erlendson, andE. Rodriguez, “Chronic Health Conditions and School Performance Among Children and Youth, ”Annals of Epidemiology23, no. 4(2013): 179–184, . doi.org/10.1016/j.annepidem.2013.01.001
- E. Delvecchio, S. Salcuni, A. Lis, A. Germani, andD. Di Riso, “Hospitalized Children: Anxiety, Coping Strategies, and Pretend Play, ”Frontiers in Public Health7(2019): 250, . doi.org/10.3389/fpubh.2019.00250
- A. Lum, C. E. Wakefield, B. Donnan, M. A. Burns, J. E. Fardell, andG. M. Marshall, “Understanding the School Experiences of Children and Adolescents With Serious Chronic Illness: A Systematic Meta‐Review, ”Child43, no. 5(2017): 645–662, . doi.org/10.1111/cch.12475
- A. Martinez‐Santos, J. D. C. Fernandez‐De‐La‐Iglesia, G. Sheaf, andI. Coyne, “A Systematic Review of the Educational Experiences and Needs of Children With Cancer Returning to School, ”Journal of Advanced Nursing77, no. 7(2021): 2971–2994, . doi.org/10.1111/jan.14784
- A. Bosch‐Alcaraz, I. Jordan, L. Benito‐Aracil, M. Á. Saz‐Roy, andA. Falcó‐Pegueroles, “Discomfort of the Critically Ill Paediatric Patient and Correlated Variables, ”Australian Critical Care33, no. 6(2020): 504–510, . doi.org/10.1016/j.aucc.2020.02.009
- K. Bsiri‐Moghaddam, M. Basiri‐Moghaddam, L. Sadeghmoghaddam, andF. Ahmadi, “The Concept of Hospitalization of Children From the View Point of Parents and Children, ”Iranian Journal of Pediatrics21, no. 2(2011): 201–208.
- C. Fuller, H. Huang, andR. Thienprayoon, “Managing Pain and Discomfort in Children With Cancer, ”Current Oncology Reports24, no. 8(2022): 961–973, . doi.org/10.1007/s11912-022-01277-1
- R. Maguire, P. Hanly, andP. Maguire, “Living Well With Chronic Illness: How Social Support, Loneliness and Psychological Appraisals Relate to Well‐Being in a Population‐Based European Sample, ”Journal of Health Psychology26, no. 10(2021): 1494–1507, . doi.org/10.1177/1359105319883923
- S. Muñoz‐Violant, V. Violant‐Holz, andM. J. Rodríguez, “Factors of Well‐Being of Youth With Complex Medical Conditions From the Experience of Hospitalization and Convalescence: A Pilot Study, ”PLoS One18, no. 5(2023): e0285213, . doi.org/10.1371/journal.pone.0285213
- M. Capurso, “Educational Options for Children With Medical Needs, ”PeerJ2(2014): e268v2, 0. 24795847 doi.org/10.7287/peerj.preprints.268v2
- N. D. Emerson, B. Distelberg, H. E. R. Morrell, J. Williams‐Reade, D. Tapanes, andS. Montgomery, “Quality of Life and School Absenteeism in Children With Chronic Illness, ”Journal of School Nursing32, no. 4(2016): 258–266, . doi.org/10.1177/1059840515615401
- A. M. Brady, J. Deighton, andS. Stansfeld, “Chronic Illness in Childhood and Early Adolescence: A Longitudinal Exploration of Co‐Occurring Mental Illness, ”Development and Psychopathology33, no. 3(2021): 885–898, . doi.org/10.1017/S0954579420000206
- K. C. Runions, R. Vithiatharan, K. Hancock, et al. , “Chronic Health Conditions, Mental Health and the School: A Narrative Review, ”Health Education Journal79, no. 4(2020): 471–483, . doi.org/10.1177/0017896919890898
- E. Alisic, “Teachers' Perspectives on Providing Support to Children After Trauma: A Qualitative Study, ”School Psychology Quarterly27, no. 1(2012): 51–59, . doi.org/10.1037/a0028590
- V. Benigno, F. Dagnino, andC. Fante, “Exploring the Impact of the COVID‐19 Pandemic on Italy's School‐In‐Hospital (SiHo) Services: The Teachers' Perspective, ”Continuity in Education1, no. 1(2020): 136–149, . doi.org/10.5334/cie.26
- L. TomberliandE. Ciucci, “Sense of School Belonging and Paediatric Illness: A Scoping Review, ”Continuity in Education2, no. 1(2021): 121–134, . doi.org/10.5334/cie.32
- L. H. Lindgren, K. Schmiegelow, A. S. Helms, T. Thorsteinsson, andH. B. Larsen, “In Sickness and in Health: Classmates Are Highly Motivated to Provide In‐Hospital Support During Childhood Cancer Therapy: In Sickness and in Health, ”Psycho‐Oncology26, no. 1(2017): 37–43, . doi.org/10.1002/pon.4094
- Hospital Organisation of Pedagogues in Europe, The Rights and Educational Needs of Children and Adolescents With Medical and Mental Health Needs (HOPE Charter), 2000, .
- M. M. Chiu, B. W. Y. Chow, C. McBride, andS. T. Mol, “Students' Sense of Belonging at School in 41 Countries: Cross‐Cultural Variability, ”Journal of Cross‐Cultural Psychology47, no. 2(2016): 175–196, . doi.org/10.1177/0022022115617031
- H. P. Libbey, “Measuring Student Relationships to School: Attachment, Bonding, Connectedness, and Engagement, ”Journal of School Health74, no. 7(2004): 274–283, . doi.org/10.1111/j.1746-1561.2004.tb08284.x
- C. D. Slaten, J. K. Ferguson, K. A. Allen, D. V. Brodrick, andL. Waters, “School Belonging: A Review of the History, Current Trends, and Future Directions, ”Educational and Developmental Psychologist33, no. 1(2016): 1–15, . doi.org/10.1017/edp.2016.6
- I. Garcia Moya, The Importance of Connectedness in Student‐Teacher Relationships: Insights From the Teacher Connectedness Project(Springer Nature, 2020).
- S. Lin, M. A. Fabris, andC. Longobardi, “Closeness in Student–Teacher Relationships and Students' Psychological Well‐Being: The Mediating Role of Hope, ”Journal of Emotional and Behavioral Disorders30, no. 1(2022): 44–53, . doi.org/10.1177/10634266211013756
- F. Zheng, “Fostering Students' Well‐Being: The Mediating Role of Teacher Interpersonal Behavior and Student‐Teacher Relationships, ”Frontiers in Psychology12(2022): 796728, . doi.org/10.3389/fpsyg.2021.796728
- K. A. Allen, C. D. Slaten, G. Arslan, S. Roffey, H. Craig, andD. A. Vella‐Brodrick, “School Belonging: The Importance of Student and Teacher Relationships, ” inThe Palgrave Handbook of Positive Education, ed. M. L. KernandM. L. Wehmeyer(Springer International Publishing, 2021), 525–550, . doi.org/10.1007/978-3-030-64537-3_21
- M. Capurso, V. Moracci, andS. Borsci, “Pathways to School Reentry for Children and Young People With a Medical or Mental Health Condition: An International Delphi Study, ”Continuing Education6, no. 1(2025): 38–57, . doi.org/10.5334/cie.159
- A. Lewandowska, B. Zych, K. Papp, et al. , “Problems, Stressors and Needs of Children and Adolescents With Cancer, ”Children8, no. 12(2021): 1173, . doi.org/10.3390/children8121173
- B. K. C. Spencer, S. Hugh‐Jones, D. Cottrell, andS. Pini, “The INSCHOOL Project: Young People With Long‐Term Physical Health Conditions: An In‐Depth Qualitative Study of Their Needs at School, ”Journal of Adolescence96, no. 2(2024): 337–349, . doi.org/10.1002/jad.12278
- K. A. AllenandM. L. Kern, School Belonging in Adolescents: Theory, Research and Practice(Springer, 2017), . doi.org/10.1007/978-981-10-5996-4
- E. J. PrinceandJ. Hadwin, “The Role of a Sense of School Belonging in Understanding the Effectiveness of Inclusion of Children With Special Educational Needs, ”International Journal of Inclusive Education17, no. 3(2013): 238–262, . doi.org/10.1080/13603116.2012.676081
- A. Gowing, “Peer‐Peer Relationships: A Key Factor in Enhancing School Connectedness and Belonging, ”Educational and Child Psychology36, no. 2(2019): 64–77, . doi.org/10.53841/bpsecp.2019.36.2.64
- V. Baskaran, L. A. Chubb, andC. B. Fouché, “Keeping Students With Long‐Term Conditions Connected With Schools: Facilitators for Sustainable Virtual Connections, ”Continuity in Education5, no. 1(2024): 111–127, . doi.org/10.5334/cie.133
- E. Ciucci, C. Facci, D. Carpenzano, et al. , “Promoting Teachers' Social and Emotional Competence in Light of the Close Connection Between Professional Role and Personal Characteristics: Preliminary Evidence of the Efficacy of the “ME4YOU” Training Program, ”IJERPH21, no. 4(2024): 511, . doi.org/10.3390/ijerph21040511
- M. Weibel, S. Skoubo, C. Handberg, et al. , “Telepresence Robots to Reduce School Absenteeism Among Children With Cancer, Neuromuscular Diseases, or Anxiety—The Expectations of Children and Teachers: A Qualitative Study in Denmark, ”Computers in Human Behavior Reports10(2023): 100280, . doi.org/10.1016/j.chbr.2023.100280
- C. Zillner, G. Rockenbauer, A. Turner, M. Röhsner, K. Klebermass‐Schrehof, andT. Pletschko, “Maintaining Health‐Related Quality of Life and Sense of Belonging for Pediatric Patients With Chronic Illnesses by Using a Telepresence Robot, ”Journal of Child Health Care30, no. 1(2026): 23–35, . doi.org/10.1177/13674935241301819
- European Commission, EU Strategy on the Rights of the Child (COM/2021/142 Final), 2021, .
- Council of Europe, Child Participation Assessment Tool, 2016, .
- S. Pini, S. Hugh‐Jones, andP. H. Gardner, “What Effect Does a Cancer Diagnosis Have on the Educational Engagement and School Life of Teenagers? A Systematic Review, ”Psycho‐Oncology21, no. 7(2012): 685–694, . doi.org/10.1002/pon.2082
- D. Maor, K. Mitchem, andR. Drewry, “The Art of Coaching: Addressing Mobile Technology Integration in a Complex Hospital School Environment, ”Continuity in Education1, no. 1(2020): 83–97, . doi.org/10.5334/cie.15
- A. E. Clarke, Situational Analysis: Grounded Theory After the Postmodern Turn(Sage Publications, 2005).
- J. Seaman, “Adopting a Grounded Theory Approach to Cultural‐Historical Research: Conflicting Methodologies or Complementary Methods?, ”International Journal of Qualitative Methods7, no. 1(2008): 1–17, . doi.org/10.1177/160940690800700101
- A. StraussandJ. Corbin, Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 2nd ed. (Sage, 1998).
- S. Sofaer, “Qualitative Methods: What Are They and Why Use Them?, ”Health Services Research34, no. 5 Pt 2(1999): 1101–1118.
- K. Darling‐McQuistan, “Beyond Representation: Exploring Drawing as Part of Children's Meaning‐Making, ”International Journal of Art and Design Education36, no. 3(2017): 281–291, . doi.org/10.1111/jade.12123
- A. Veale, “Creative Methodologies in Participatory Research With Children, ” inResearching Children's Experience: Approaches and Methods(Sage, 2005), 253–272.
- E. L. Holliday, L. J. Harrison, andS. McLeod, “Listening to Children With Communication Impairment Talking Through Their Drawings, ”Journal of Early Childhood Research179, no. 4(2009): 463–474, . doi.org/10.1080/03004430701379195
- C. Branquinho, C. Kelly, L. C. Arevalo, A. Santos, andM. Gaspar De Matos, ““Hey, We Also Have Something to Say”: A Qualitative Study of Portuguese Adolescents' and Young People's Experiences Under COVID‐19, ”Journal of Community Psychology48, no. 8(2020): 2740–2752, . doi.org/10.1002/jcop.22453
- M. Capurso, L. Buratta, andC. Mazzeschi, “Primary and Middle‐School Children's Drawings of the Lockdown in Italy, ”Frontiers in Psychology13(2022): 982654, . doi.org/10.3389/fpsyg.2022.982654
- N. Idoiaga, N. Berasategi, A. Eiguren, andM. Picaza, “Exploring Children's Social and Emotional Representations of the COVID‐19 Pandemic, ”Frontiers in Psychology11(2020): 1952, . doi.org/10.3389/fpsyg.2020.01952
- L. S. Nowell, J. M. Norris, D. E. White, andN. J. Moules, “Thematic Analysis: Striving to Meet the Trustworthiness Criteria, ”International Journal of Qualitative Methods16, no. 1(2017): 1609406917733847, . doi.org/10.1177/1609406917733847
- K. Ring, “What Mothers Do: Everyday Routines and Rituals and the Meaning of Drawing, ”International Journal of Art and Design Education25, no. 2(2006): 205–214, . doi.org/10.1111/j.1476-8070.2006.00493.x
- J. Einarsdottir, “Research With Children: Methodological and Ethical Challenges, ”European Early Childhood Education Research Journal15, no. 2(2007): 197–211, . doi.org/10.1080/13502930701321477
- K. Charmaz, Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis(Sage Publications, 2006).
- B. G. GlaserandA. L. Strauss, The Discovery of Grounded Theory: Strategies for Qualitative Research(Aldine Publishing, 1967).
- E. Ciucci, L. Tomberli, E. Amore, A. Smorti, F. Maffei, andL. Vagnoli, “The Effects of Hospital‐Based School Lessons on Children's Emotions, Distress and Pain, ”Continuity in Education5, no. 1(2024): 100–110, . doi.org/10.5334/cie.118
- S. R. ShawandP. C. McCabe, “Hospital‐To‐School Transition for Children With Chronic Illness: Meeting the New Challenges of an Evolving Health Care System, ”Psychology in the Schools57, no. 7(2020): 1040–1052, . doi.org/10.1002/pits.22368
- D. Thompson, Schooling in the Hospital: Supporting Children's Learning During Illness(Routledge, 2016).
- M. Capurso, G. Catalano, A. Calvaruso, et al. , “Tailored Psychoeducational Home Interventions for Children With a Chronic Illness: Families and Experiences, ”CiE5, no. 1(2024): 1–21, . doi.org/10.5334/cie.100
- B. K. HamreandR. C. Pianta, “Can Instructional and Emotional Support in the First‐Grade Classroom Make a Difference for Children at Risk of School Failure?, ”Child Development76, no. 5(2005): 949–967, . doi.org/10.1111/j.1467-8624.2005.00889.x
- R. C. Pianta, Enhancing Relationships Between Children and Teachers(American Psychological Association, 1999), . doi.org/10.1037/10314-000
- V. Benigno, G. P. Caruso, F. M. Dagnino, E. Dalla Mutta, andC. Fante, “Enhancing Home Education in Italian Context: Teachers' Perception of a Hybrid Inclusive Classroom, ”Education in Science12, no. 8(2022): 563, . doi.org/10.3390/educsci12080563
- J. M. Fegert, B. Vitiello, P. L. Plener, andV. Clemens, “Challenges and Burden of the Coronavirus 2019 (COVID‐19) Pandemic for Child and Adolescent Mental Health: A Narrative Review to Highlight Clinical and Research Needs in the Acute Phase and the Long Return to Normality, ”Child and Adolescent Psychiatry and Mental Health14, no. 1(2020): 20, . doi.org/10.1186/s13034-020-00329-3
- K. A. AllenandT. Bowles, “Belonging as a Guiding Principle in the Education of Adolescents, ”Australian Journal of Educational and Developmental Psychology12(2012): 108–119.
- C. Goodenow, “Classroom Belonging Among Early Adolescent Students: Relationships to Motivation and Achievement, ”Journal of Early Adolescence13, no. 1(1993): 21–43, . doi.org/10.1177/0272431693013001002
- L. Hopkins, “Hospital Education: Supporting Children's Learning and Belonging During Illness, ” inThe Handbook of Educational Inclusion, ed. S. Taylor(Routledge, 2018), 233–248.
- R. F. BaumeisterandM. R. Leary, “The Need to Belong: Desire for Interpersonal Attachments as a Fundamental Human Motivation, ”Psychological Bulletin117, no. 3(1995): 497–529, . doi.org/10.1037/0033-2909.117.3.497
- R. M. RyanandE. L. Deci, “Self‐Determination Theory and the Facilitation of Intrinsic Motivation, Social Development, and Well‐Being, ”American Psychologist55, no. 1(2000): 68–78, . doi.org/10.1037/0003-066X.55.1.68
- S. R. ShawandP. C. McCabe, “Hospital‐To‐School Transition for Children With Chronic Illness: Meeting the New Challenges of an Evolving Health Care System, ”Psychology in the Schools45, no. 1(2008): 74–87.
- V. A. Newhart, “Assistive Technology in the Classroom: The Use of Telepresence Robots to Support Inclusion of Students With Disabilities, ”Assistive Technology Outcomes and Benefits8, no. 1(2014): 1–15.
- E. Soares, M. Rodrigues, andA. Rocha, “Using Telepresence Robots to Support School Participation of Hospitalized Children, ”International Journal of Medical Informatics107(2017): 41–50, . doi.org/10.1016/j.ijmedinf.2017.08.003
- R. M. Yilmaz, F. B. Topu, andY. Goktas, “Using Mobile Technologies in Hospital Classrooms: Effects on Student Engagement and Learning, ”Computers in Education79(2014): 87–96, . doi.org/10.1016/j.compedu.2014.07.009
- C. J. Kaffenberger, “School Reentry for Students With a Chronic Illness: A Role for Professional School Counselors, ”Professional School Counseling16, no. 1(2012): 1–10.
Republished from the open web under CC-BY. Authors: Tomberli L, Vagnoli L, Pavone L, Amore E, Ciucci E. Read the original.